
A Health Assessment Form is an essential tool for gathering information related to a patient’s health status. This guide offers a comprehensive overview, complete with practical examples to ensure efficient evaluations. By using an Assessment Form or Initial Assessment Form, medical professionals can accurately document vital health details. This process aids in detecting potential risks, planning treatments, and tailoring care based on specific patient needs. Whether used in clinics, hospitals, or other healthcare facilities, having a well-structured health assessment form helps maintain a standardized approach to patient care and ensures effective communication between medical staff.
Download Health Assessment Form Bundle
What is Health Assessment Form?
A Health Assessment Form is a structured document used to collect comprehensive information about an individual’s health. It typically includes medical history, current conditions, lifestyle habits, and symptoms. This form is crucial for healthcare professionals to understand a patient’s health profile, aiding in diagnosis, treatment planning, and preventive measures. By standardizing health data collection, these forms help ensure consistent and accurate medical records
Health Assessment Format
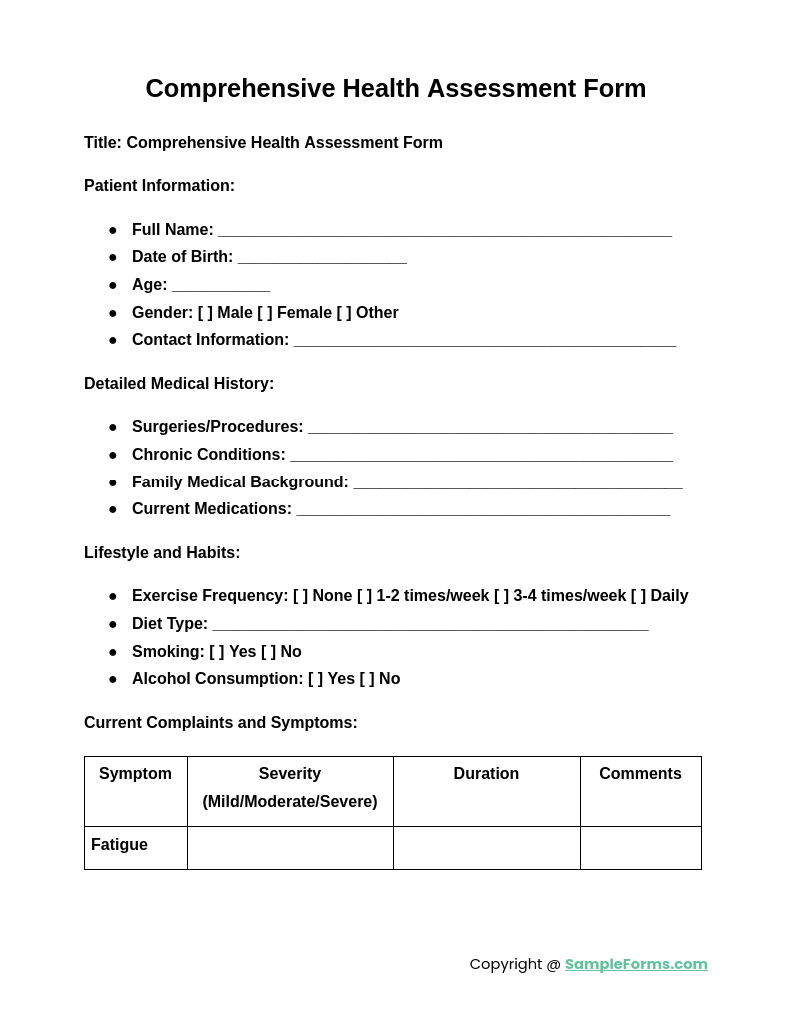
Title: Comprehensive Health Assessment Form
Patient Information:
- Full Name: ______________________________________________
- Date of Birth: ___________________
- Age: ___________
- Gender: [ ] Male [ ] Female [ ] Other
- Contact Information: _______________________________________
- Address: ____________________________________________________
Medical History:
- Past Surgeries: ____________________________________________
- Chronic Conditions (e.g., diabetes, hypertension): ______________
- Family Medical History: _____________________________________
- Known Allergies: ___________________________________________
Current Symptoms and Concerns:
- Primary Complaint: ________________________________________
- Duration of Symptoms: _____________________________________
- Associated Symptoms: ______________________________________
Lifestyle and Habits:
- Smoking: [ ] Yes [ ] No
- Alcohol Consumption: [ ] Yes [ ] No
- Physical Activity (Frequency/Type): __________________________
- Diet Type: _________________________________________________
Medications and Treatments:
- Current Medications: _______________________________________
- Recent Treatments or Therapies: _____________________________
Physician/Assessor Notes:
- Observations: _____________________________________________
- Recommendations: _________________________________________
Physician’s Name and Signature: _____________________________
Date: ___________________
Health Assessment Form Nursing
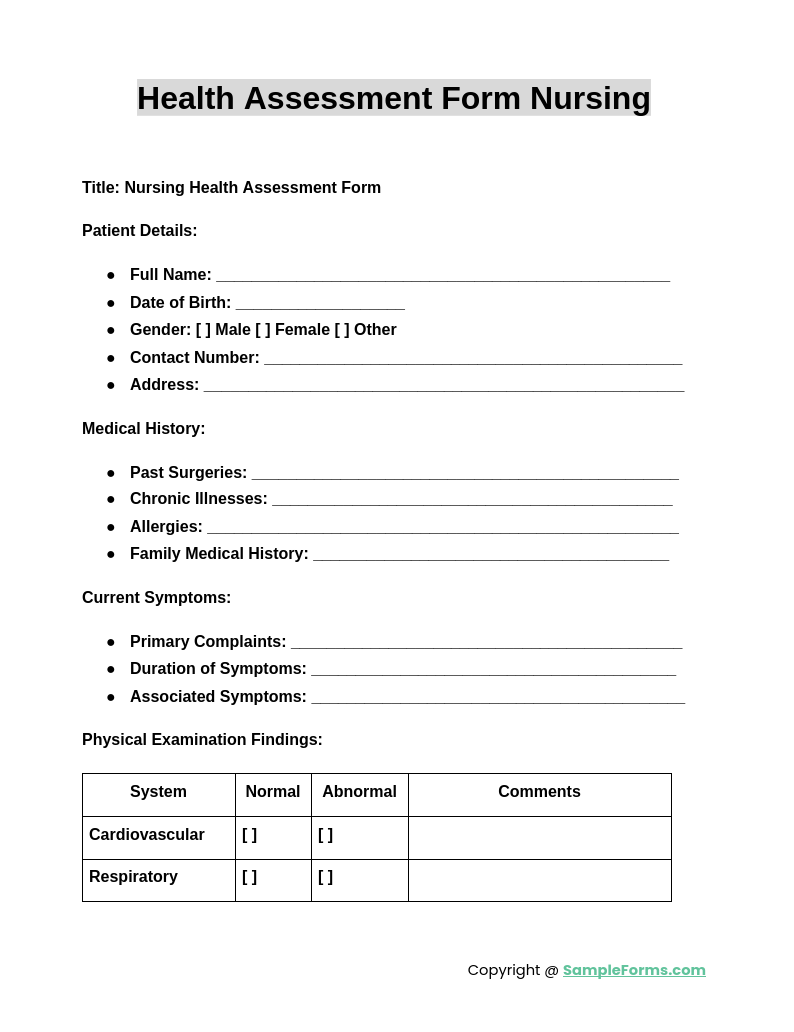
A Health Assessment Form Nursing is vital for collecting patient data during medical evaluations. It helps nurses document health history, symptoms, and vital signs efficiently. Utilize a Nursing Assessment Form for thorough, consistent, and accurate patient records.
Employee Health Assessment Form
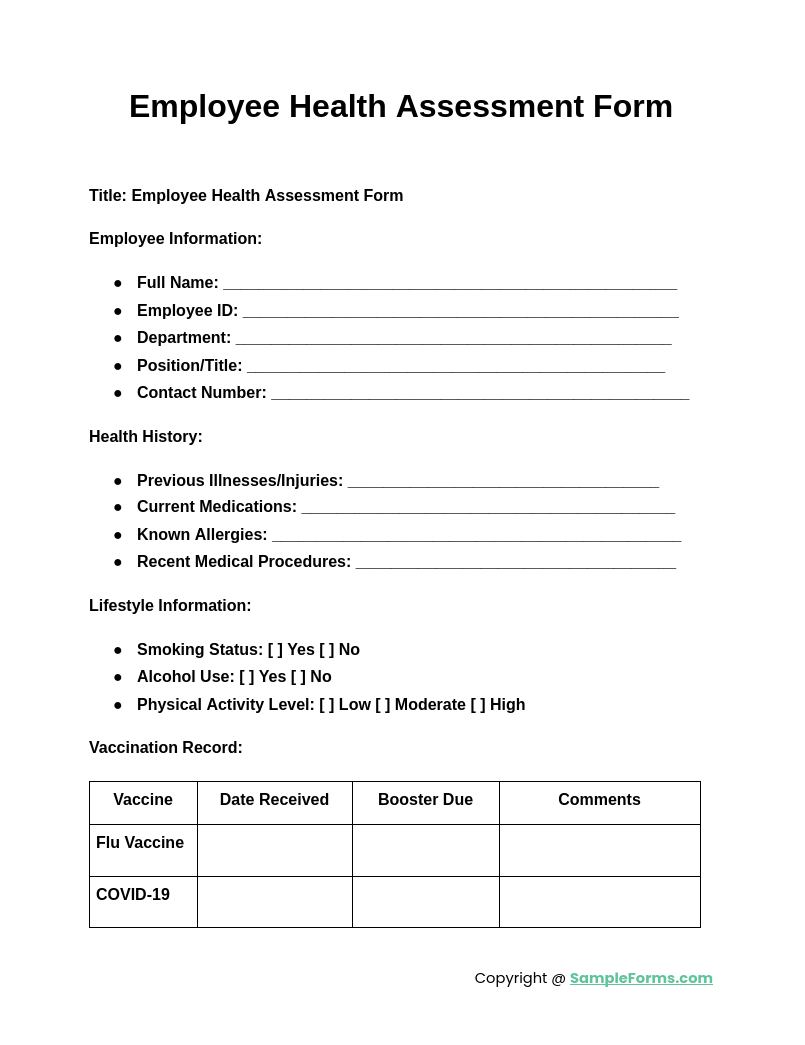
An Employee Health Assessment Form ensures the well-being of staff by tracking health status and identifying risks. This aids in promoting a healthy work environment and safety. It complements other evaluation tools like an Interview Assessment Form for comprehensive records.
Health Assessment Form for School
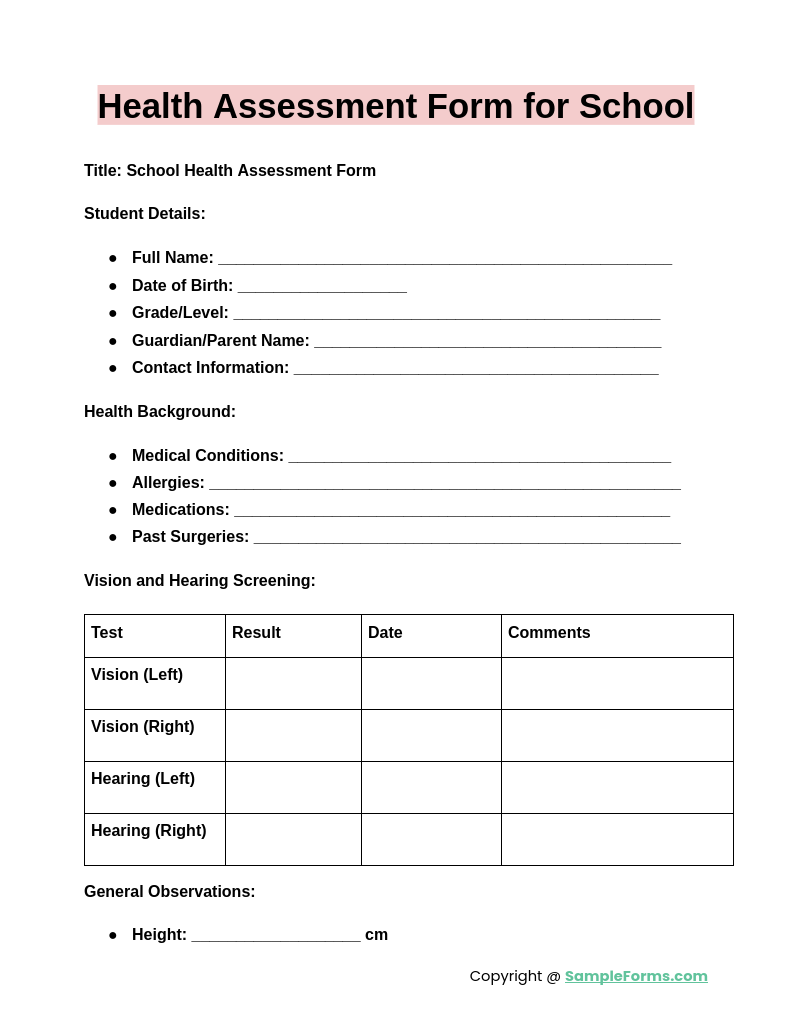
A Health Assessment Form for School is essential for monitoring student health and identifying potential issues. This form captures medical history, vaccinations, and allergies, ensuring a safe learning environment. It pairs well with Physical Therapy Assessment Form for specialized care.
Comprehensive Health Assessment Form
A Comprehensive Health Assessment Form provides a detailed overview of a patient’s physical and mental health. It includes medical history, lifestyle, and risk factors. Use it alongside a Fitness Assessment Form to address overall well-being and preventative care.
Browse More Health Assessment Forms
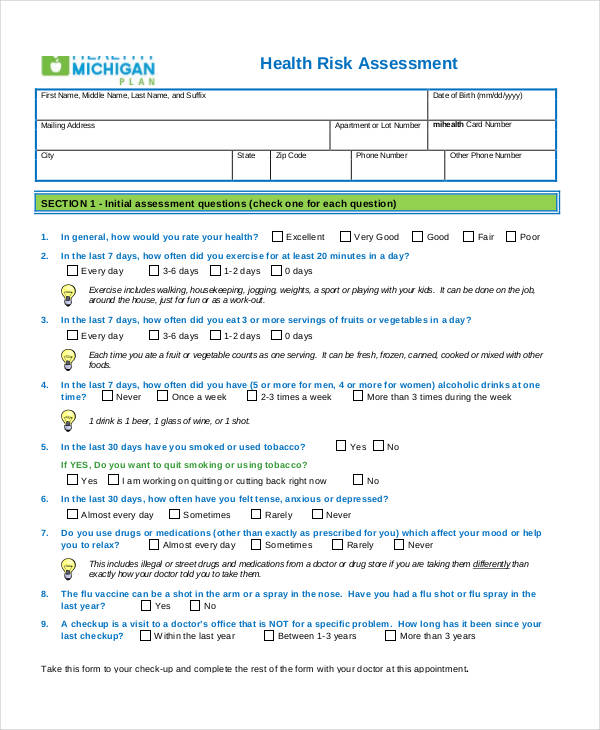
Personal Health Risk Assessment Form
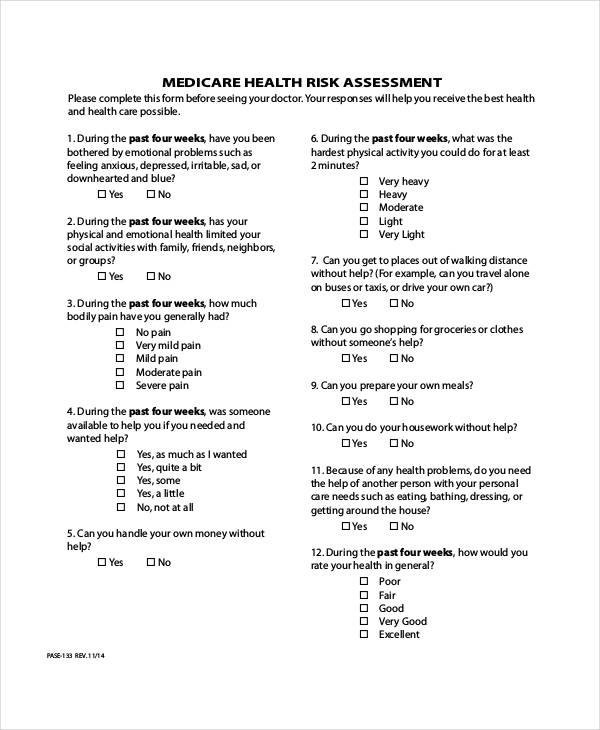
Medicare Health Risk Assessment Form
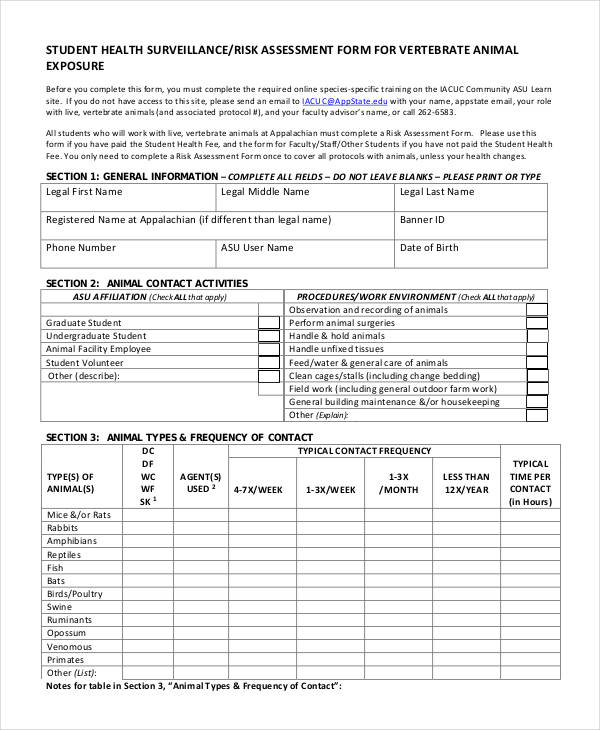
Health Surveillance Risk Assessment Form
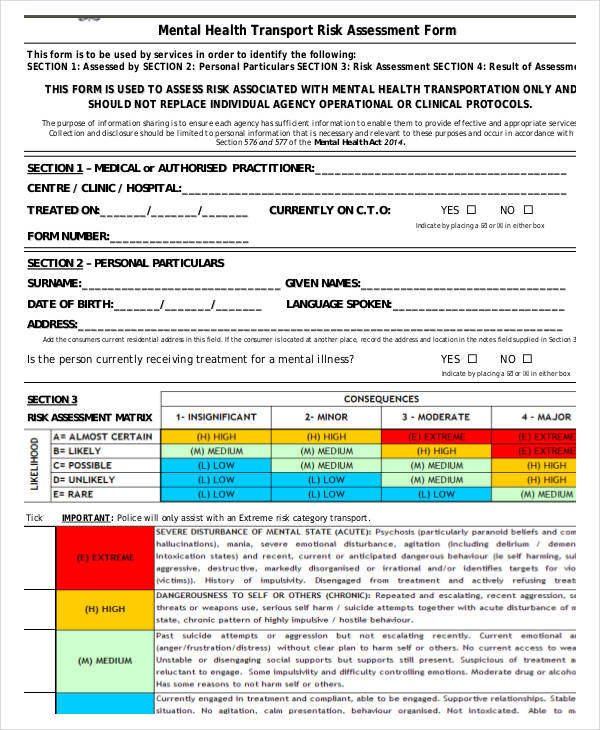
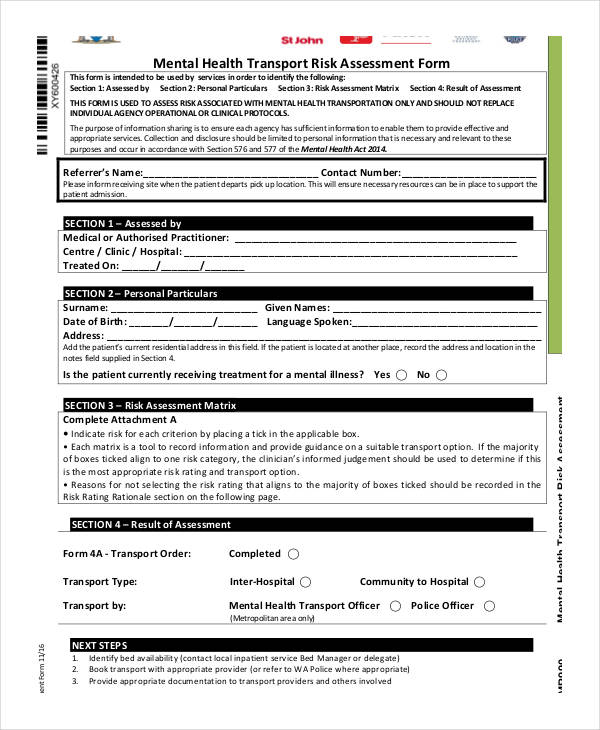
Mental Health Transport Risk Assessment Form
Medicare Health Assessment Forms
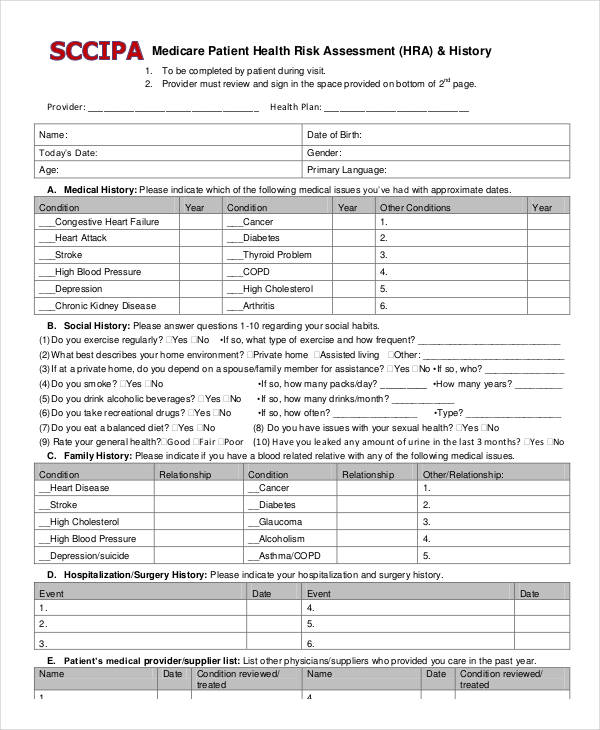
Medicare Patient Health Risk Assessment Form
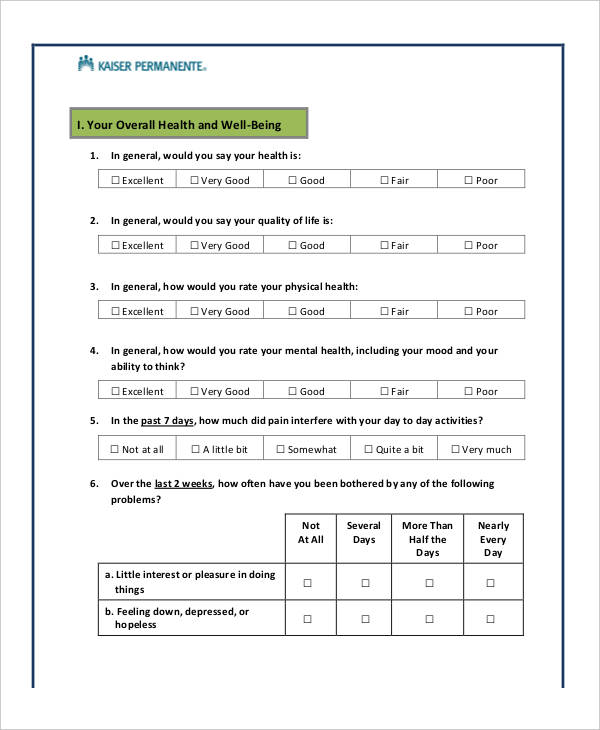
Medicare Health Assessment Questionnaire Form
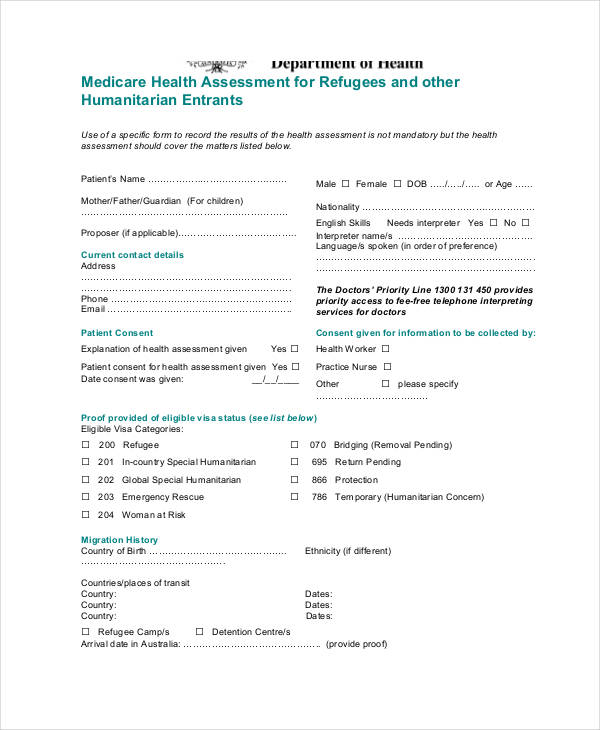
Medicare Refugee Health Assessment Form
Medicare Annual Wellness Health Assessment Form
Nursing Health Assessment Forms
Nursing Health and Safety Assessment Form
Nursing Health Questionnaire Assessment Form
Nursing Care Health Assessment Form
Child Health Assessment Forms
Child Care Staff Health Assessment Form
Child Health Assessment Form Example
Child Development Center Health Assessment Form
Child and Youth Services Health Assessment Form
Mental Health Assessment Forms
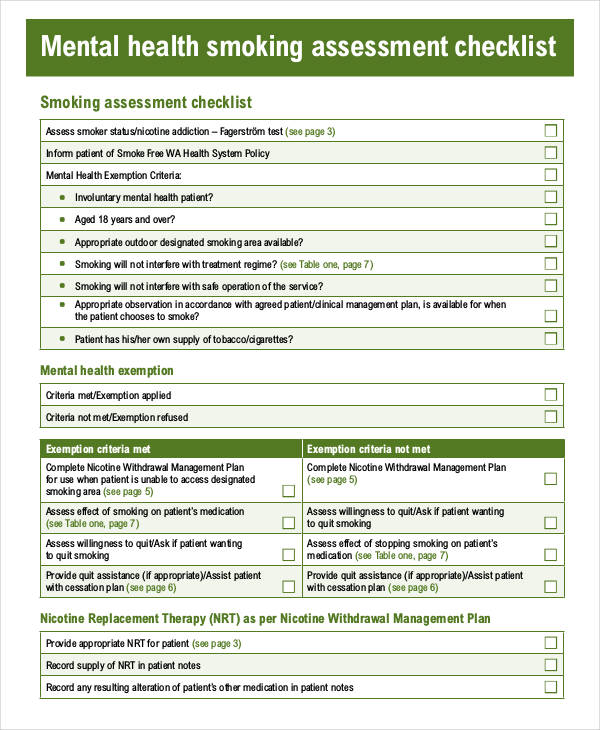
Mental Health Assessment Checklist Form
Mental Health Transport Risk Assessment Form
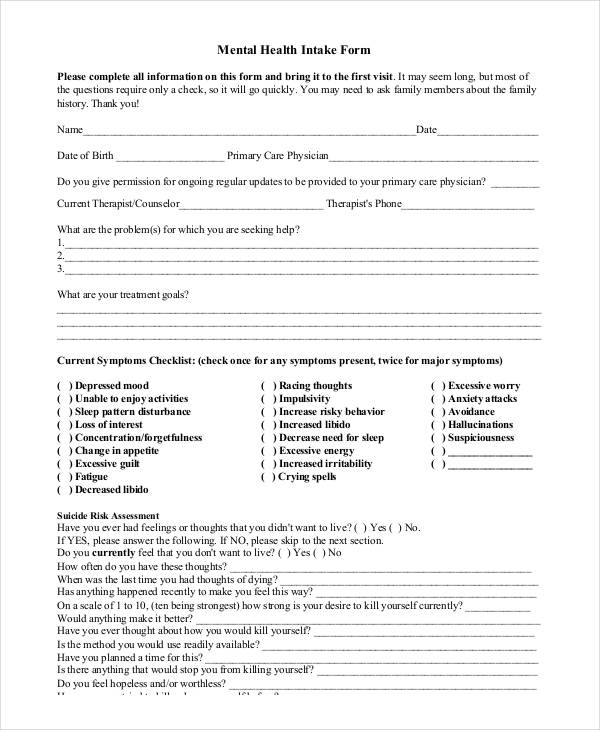
Mental Health Intake Assessment Form
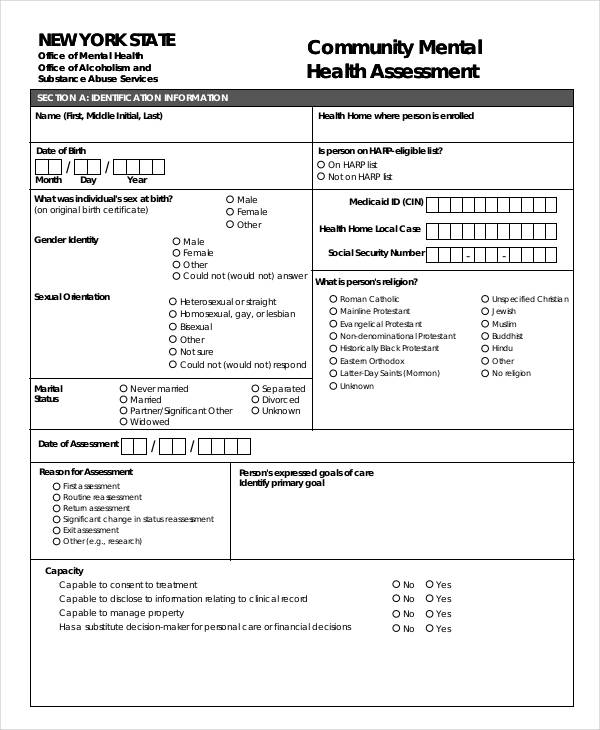
Community Mental Health Assessment Form
Physical Health Assessment Forms
Mental Health Physical Assessment Form
Health Care Physical Assessment Form
Health and Safety Risk Assessment Forms
Maternity Health and Safety Risk Assessment Form
Blank Health and Safety Risk Assessment Form
Event Health and Safety Risk Assessment Form
General Health and Safety Risk Assessment Form
Annual Health Assessment Forms
Annual Senior Health Assessment Form
Annual Employment Health Assessment Form
School Health Assessment Forms
School Nurse Health Assessment Form
School Entry Health Assessment Form
School District Health Assessment Form
Preschool Health Assessment Form
Health Assessment Record Forms
Initial Health Assessment Record Form
Early Childhood Health Assessment Record Form
Oral Health Assessment Forms
Oral Health Risk Assessment Form
Oral Health Assessment/Waiver Request Form
Initial Health Assessment Forms
Initial Mental Health Assessment Form
Initial Behavioral Health Assessment Form
Initial Pediatric Health Assessment Form
Mental Health Assessment Sample
What are the types of health assessment?
The types of health assessment cater to different aspects of patient health for a comprehensive understanding. Types include:
- Initial Assessment: A broad overview conducted during the first visit.
- Focused Assessment: Centers on a specific issue, like a Functional Behavior Assessment Form.
- Comprehensive Assessment: A detailed evaluation covering all health areas.
- Ongoing Assessment: Continuous monitoring for treatment progress.
- Specialized Assessment: Targeted evaluations, such as a Skills Assessment Form, for specific functions or conditions.
What are the 5 steps of health assessment?
The 5 steps of health assessment ensure a comprehensive evaluation of a patient’s health status for effective care. Key steps include:
- Patient History Collection: Gather past and present health history using tools like a Psychosocial Assessment Form.
- Physical Examination: Conduct a thorough examination to identify physical symptoms and potential health issues.
- Observation: Note non-verbal cues that may indicate underlying conditions, such as distress or discomfort.
- Data Analysis: Analyze collected information to identify patterns and potential health risks.
- Documentation: Record all findings accurately to inform future assessments and treatments.
How to fill out a health assessment form?
Filling out a health assessment form requires careful attention to ensure accurate and comprehensive information. Follow these steps:
- Read Instructions: Understand the form requirements, such as for a Nutrition Assessment Form.
- Personal Details: Provide accurate demographic data, including name and contact information.
- Health History: Complete all sections related to past illnesses, allergies, and treatments.
- Current Symptoms: Clearly describe any present symptoms or concerns.
- Review and Submit: Double-check the form for completeness before submission.
What are the 5 purposes of health assessment?
The 5 purposes of health assessment highlight its importance in patient care and overall well-being. Key purposes include:
- Baseline Data Collection: Establish initial data to monitor health changes over time.
- Diagnosis: Aid in identifying conditions through tools like a Mental Health Assessment Form.
- Treatment Planning: Formulate personalized treatment plans based on collected data.
- Monitoring Progress: Assess the effectiveness of current treatment or interventions.
- Prevention: Detect early signs of potential health issues to prevent complications.
What are the 4 techniques of health assessment?
The 4 techniques of health assessment ensure a thorough evaluation of a patient’s condition for accurate diagnoses. The techniques include:
- Inspection: Visually examine the patient for any abnormalities or changes.
- Palpation: Use hands to feel body structures and detect issues.
- Percussion: Tap on specific areas to hear sounds that indicate organ conditions.
- Auscultation: Listen to body sounds using a stethoscope, essential for assessing heart and lung function. You may also see Wellness Assessment Form
What is a health assessment in PPT?
A health assessment in PPT is a presentation format summarizing health evaluations, processes, and outcomes. It can be customized for various purposes, such as explaining a Community Assessment Form during professional or educational workshops.
How to do a full body assessment?
A full body assessment checks overall health, including vitals, physical examination, and history review. Use a structured Pre Training Assessment Form for systematic documentation, ensuring comprehensive patient evaluation.
What is a general health assessment?
A general health assessment evaluates a person’s overall health status, including medical history, physical exam, and lifestyle analysis. It supports proactive healthcare and can align with tools like a Child Assessment Form for thorough tracking.
What are the health assessment questions?
Health assessment questions include inquiries about medical history, current symptoms, lifestyle habits, and mental well-being. These questions help healthcare providers collect comprehensive data for creating Client Assessment Form documentation.
What is project health assessment?
A project health assessment evaluates a project’s progress, risks, and overall condition to ensure goals are met effectively. This process is similar in approach to an Army Risk Assessment Form for safety evaluations.
What is assessment of health status?
Assessment of health status refers to evaluating an individual’s physical, mental, and emotional health through systematic data collection. This includes using a Capacity Assessment Form for specific condition analysis.
What is a health assessment tool?
A health assessment tool aids in measuring and documenting health indicators such as vitals, symptoms, and patient history. It supports comprehensive assessments and can complement a Driver Assessment Form for specific use cases.
What is a basic health test?
A basic health test includes simple evaluations like blood pressure, heart rate, and blood work. These tests can be part of a routine or a targeted check, similar to a Fall Risk Assessment Form.
What is the health assessment method?
The health assessment method involves steps like history taking, physical exams, and observation. This structured approach ensures thorough patient evaluation, comparable to filling out a Family Assessment Form for context.
What is the NC health assessment form?
The NC health assessment form is used in North Carolina to document student health for school entry. It collects medical history, vaccinations, and screenings, aligning with practices like a Hazard Assessment Form for thorough checks.
In conclusion, a Health Assessment Form: Sample, Forms, Letters, Use is a crucial tool in healthcare for obtaining detailed patient information and guiding care plans. This comprehensive document enables medical professionals to make informed decisions, ensuring patients receive accurate and effective care. Utilizing a structured format like a Management Risk Assessment Form supports consistent data collection, helping practitioners detect early warning signs and prevent potential issues. Implementing health assessment forms as a standard practice promotes better patient outcomes and improved communication among healthcare teams.
Related Posts
-
How to Appeal Medical Assessment Verdict? [ What Is, How Do ]
-
5 Assessment Methods That Promote Content Retention
-
Enquiry Form
-
FREE 5+ Recruiter Performance Review Forms in PDF | MS Word
-
Job Safety Observation Form
-
FREE 4+ Hazard Observation Forms in PDF
-
FREE 5+ Coach Observation Forms in PDF | MS Word
-
FREE 4+ Child Care Observation Forms in MS Word | PDF
-
FREE 4+ Child Observation Forms in PDF | MS Word
-
Preschool Observation Form
-
Student Observation Form
-
Peer Observation Form
-
Lesson Observation Form
-
Content Retention Through Assessment Form [ How to, Importance, Tips ]
-
The Importance of Risk Assessment and Safety Statement [ What Is, How to Conduct ]