
A Nursing Assessment Form is a critical tool in patient care, allowing nurses to document health status and plan appropriate interventions. This comprehensive guide provides everything you need to know about creating and using an Assessment Form effectively. Learn how to structure forms to include vital information such as patient history, current health status, and care plans. With practical examples and tips, this guide ensures you can develop an efficient and thorough Self Assessment process, enhancing patient outcomes and nursing efficiency.
Download Nursing Assessment Form Bundle
What is Nursing Assessment Form?
A Nursing Assessment Form is a structured document used by nurses to gather comprehensive information about a patient’s health status. This Assessment Form includes sections for recording medical history, physical examination findings, and current symptoms. It serves as a foundation for developing a personalized care plan and ensuring thorough, continuous patient evaluation.
Nursing Assessment Format
Title: Nursing Assessment Form
Section 1: Patient Information
- Full Name:
- Date of Birth:
- Address:
- Contact Number:
- Emergency Contact Information:
Section 2: Health History
- Medical History:
- Current Medications:
- Allergies:
- Recent Surgeries:
Section 3: Physical Assessment
- Vital Signs:
- Pain Assessment:
- Mobility Status:
- Nutrition and Hydration:
Section 4: Nursing Diagnosis
- Identified Problems:
- Recommended Interventions:
Section 5: Care Plan
- Goals:
- Planned Interventions:
- Follow-up Schedule:
Section 6: Nurse’s Notes
- Additional Observations:
- Nurse’s Signature:
- Date:
Nursing Assessment Form PDF
A Nursing Assessment Form PDF provides a standardized, digital format for documenting patient evaluations. Easily accessible and printable, it ensures consistency and thoroughness in assessments, similar to a Risk Assessment Form used for safety evaluations.
Free Printable Nursing Assessment Form
A Free Printable Nursing Assessment Form offers a cost-effective solution for nurses to document patient health status. This form is readily available for download, ensuring comprehensive care, much like a Nursing Feedback Form collects essential feedback.
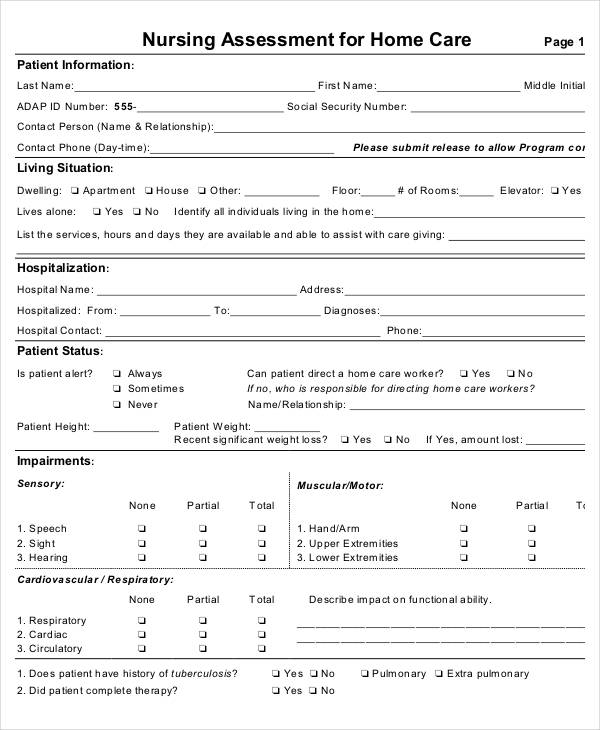
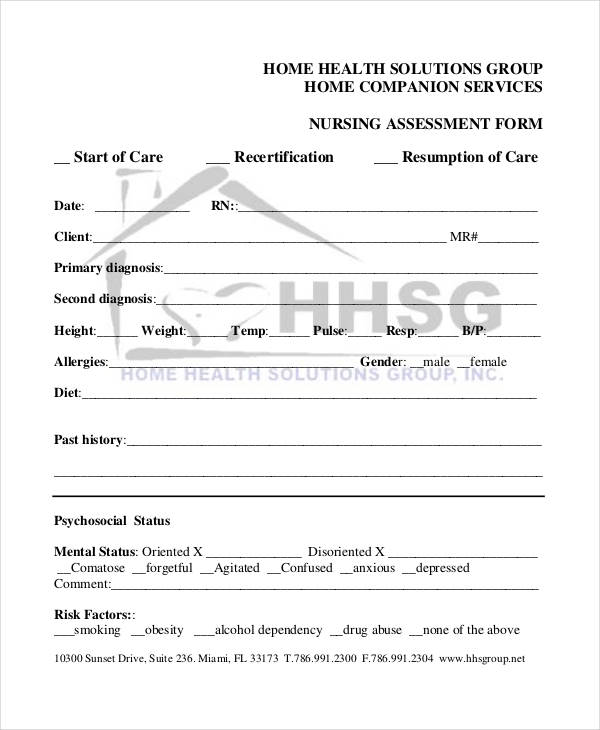
Nursing Assessment Form for Home Care
A Nursing Assessment Form for Home Care is designed to assess patients in their home environment. This form includes detailed sections for medical history, current health status, and care plans, similar to a Nursing Audit Form used for quality checks.
Nursing Initial Assessment Form
The Nursing Initial Assessment Form is crucial for the first evaluation of a new patient. It gathers comprehensive information on medical history, physical examination, and current symptoms, ensuring a thorough baseline assessment, akin to a Nursing Registration Form for new patients.
More Nursing Assessment Form Samples
Nursing Physical Assessment Form
School Nursing Physical Assessment Form
Nursing Admission Assessment Forms
Pediatric Nursing Admission Assessment
Hospital Nursing Admission Form
Nursing Health Assessment Forms
Nursing Care Health Assessment Form
Nursing Initial Health Assessment Form
Nurses and Doctors Working Together
When one is asked to think of people associated to the medical field, a doctor or nurse comes to mind. These two medical professionals are commonly known by all are the two people a person is likely to encounter in a hospital. They are also known to work together in any medical emergency like accidents, medical procedures such as surgery, medical processes such as the completion of Physical Assessment Form.
Collaborative care is the term in describing the working relationship of a nurse and a doctor. A nurse and doctor have their own set of responsibilities but are able to help each other.
Comprehensive Nursing Assessment Forms
Sample Comprehensive Nursing Assessment
Resident Comprehensive Nursing Form
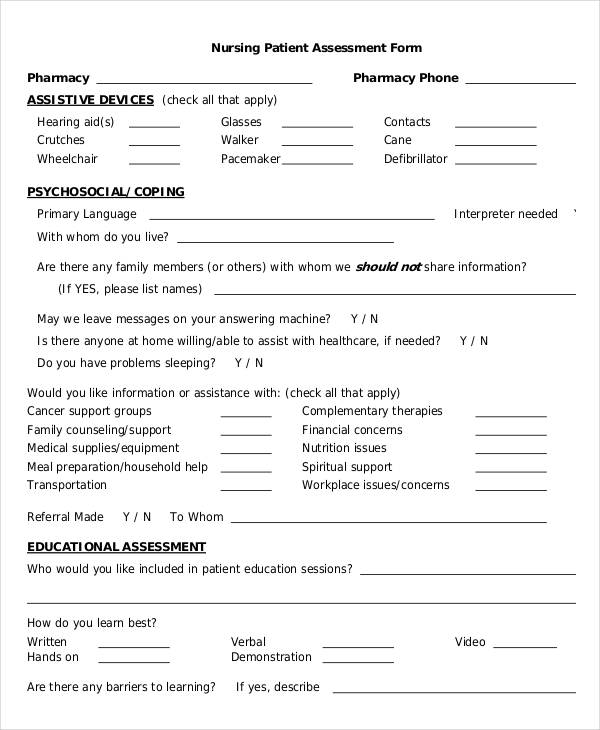
Nursing Patient Assessment Forms
Nursing Patient Assessment Example
Pharmacy Nursing Patient Assessment Form
 health.ny.gov
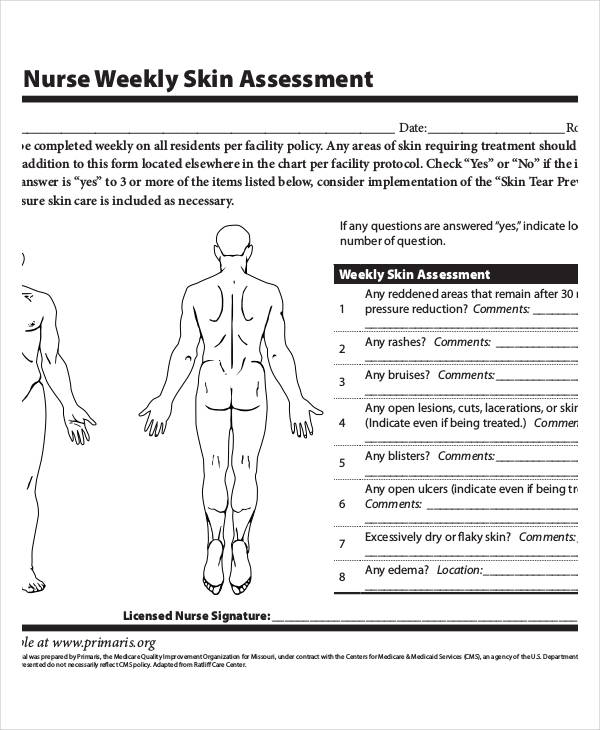
health.ny.govNursing Skin Assessment Forms
Nursing Weekly Skin Assessment
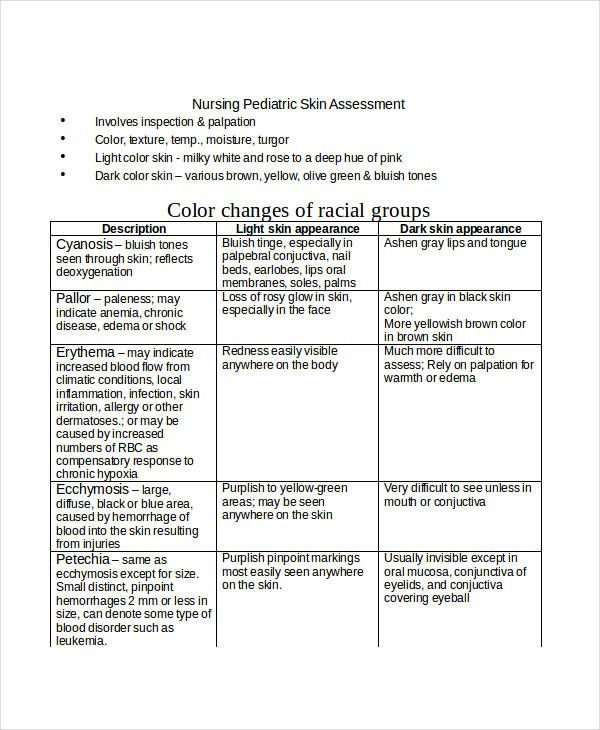
Nursing Pediatric Skin Assessment in Doc
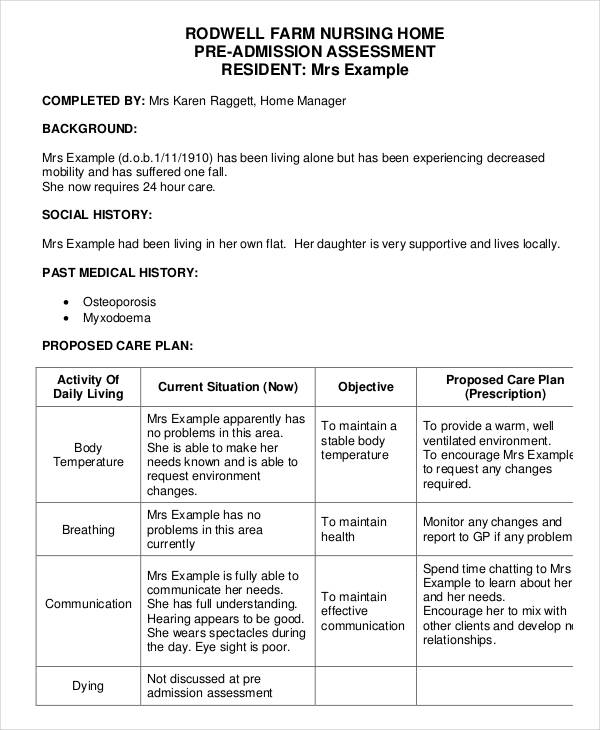
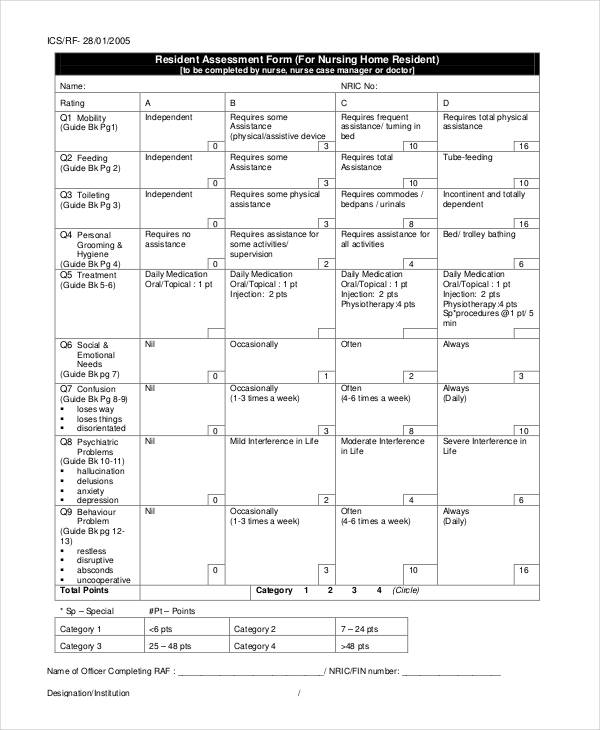
Nursing Home Assessment Forms
Nursing Home Pre-Admission Assessment Form
Nursing Home Resident Assessment Form
Nursing Home Assessment Form in Doc

Free Nursing Assessment Forms
Nursing Assessment Form Example
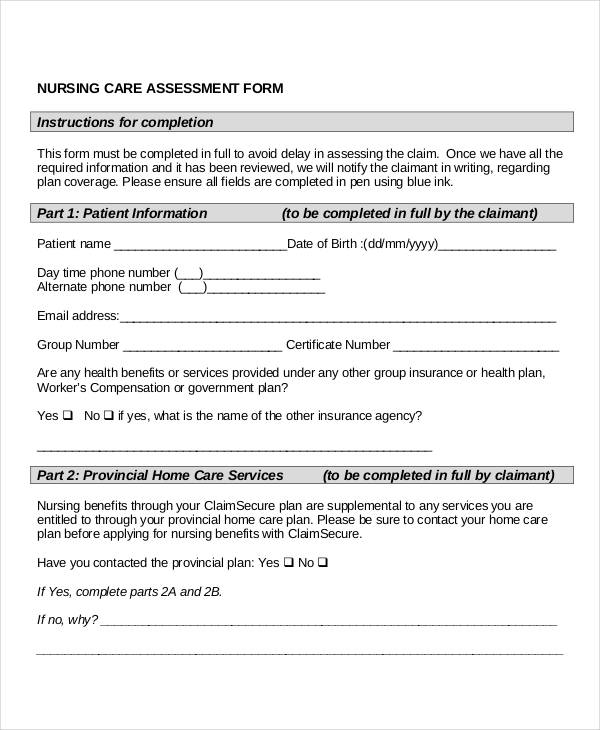
Nursing Care Assessment Form
Nursing Adult Assessment Forms
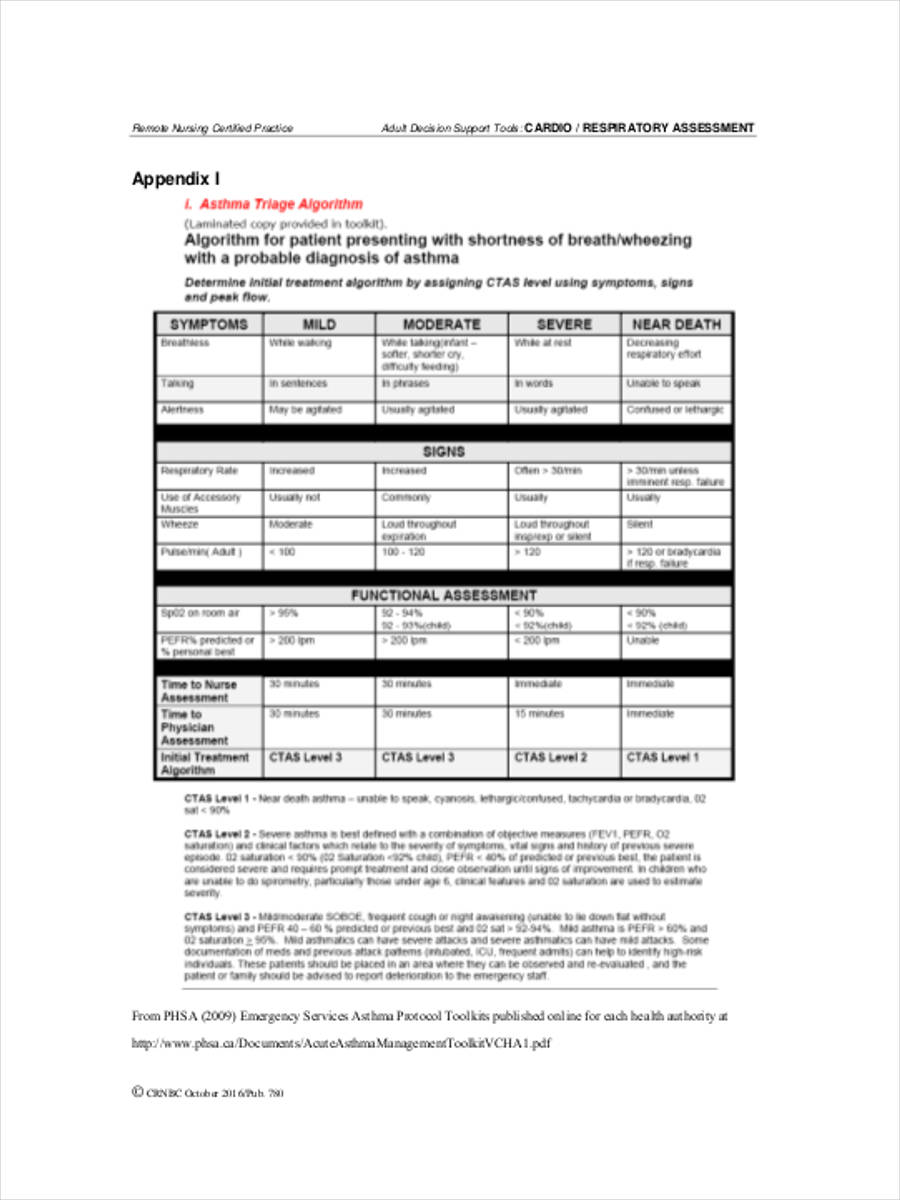
Nursing Adult Respiratory Assessment
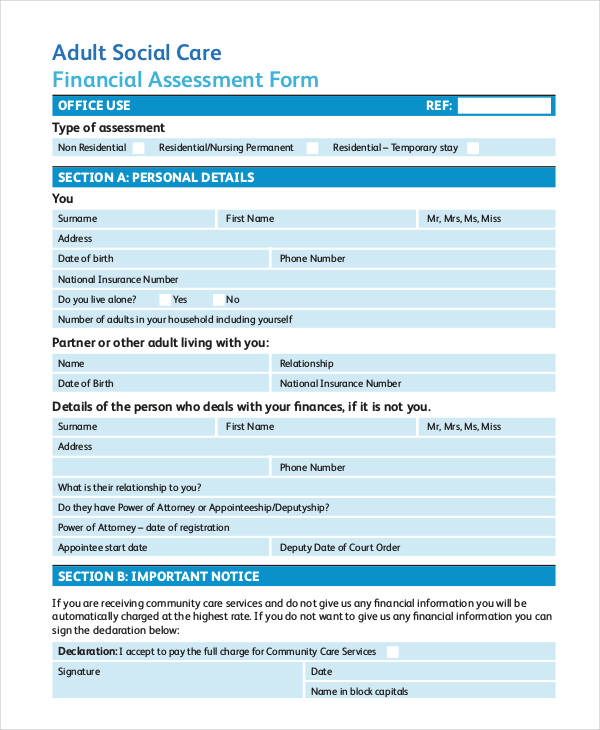
Social Care Nursing Adult Assessment Form
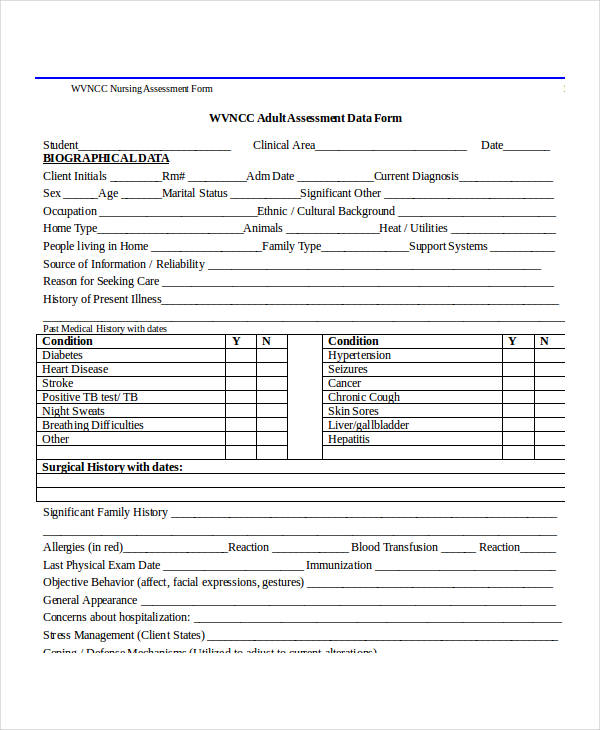
Nursing Adult Health Assessment in Doc
What are the 5 major steps in nursing assessment?
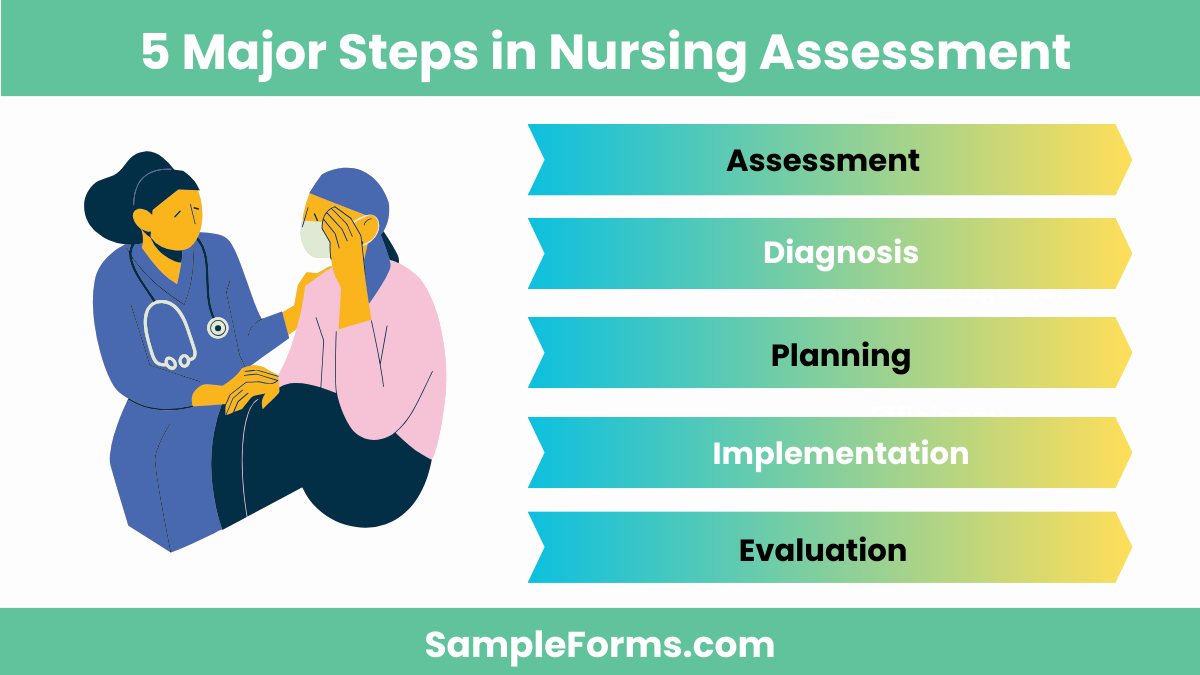
Nursing assessment involves a systematic approach to gather comprehensive patient information. Key steps include:
- Assessment: Collecting patient data through observation and interviews, similar to using an Interview Assessment Form.
- Diagnosis: Analyzing data to identify health issues.
- Planning: Developing a care plan with specific goals.
- Implementation: Executing the care plan.
- Evaluation: Assessing the effectiveness of the care plan. You may also see Mental Health Assessment Form
What is the purpose of a nursing assessment?
A nursing assessment aims to understand a patient’s health status and needs. Key purposes include:
- Identify Health Issues: Detect potential or existing health problems.
- Plan Care: Develop personalized care plans, like a Physical Therapy Assessment Form.
- Monitor Progress: Track patient progress and adjust care as needed.
- Communication: Facilitate communication among healthcare providers.
- Document Care: Ensure accurate and comprehensive patient records.
What are the different types of nursing assessment?
Nursing assessments vary based on the patient’s condition and care setting. Key types include:
- Initial Assessment: Comprehensive evaluation upon admission.
- Focused Assessment: Specific to a particular issue or symptom, similar to a Fitness Assessment Form.
- Emergency Assessment: Quick evaluation during emergencies.
- Time-Lapsed Assessment: Periodic re-evaluation to monitor changes.
- Functional Assessment: Evaluating a patient’s ability to perform daily activities.
What are the 4 P’s of nursing assessment?
The 4 P’s of nursing assessment are essential elements for patient evaluation. Key components include:
- Pain: Assessing the presence and intensity of pain.
- Position: Evaluating the patient’s position and comfort.
- Personal Needs: Identifying personal care needs, akin to a Psychosocial Assessment Form.
- Preventive Measures: Implementing measures to prevent complications.
Tips in Interviewing a Patient
A diagnosis and treatment are heavily dependent on the information disclosed by the patient. This type of information can be gathered through a number of ways and methods. One of the methods that has incorporated into a doctor’s daily routine and overall hospital protocol is the the administration of assessment forms. You may also see Functional Behavior Assessment Form
The form distributed can vary from a Medical Assessment Form to a Psychosocial Assessment Forms. This method may be reliable since it contains a standardized format but there are other methods that gather even more information from a patient. A method that can achieve this objective is the interview method. You may also see Business Assessment Form
An interview would involve the patient and doctor having a face to face conversation about the patient’s current health needs. The interview may go sour if the doctor, nurse, or delegated medical personnel does not utilize the method to its fullest potential. You may also see Candidate Assessment Form
For the interview to go well, rapport must be established between the doctor and the patient. This is done in order for the patient to feel comfortable. Another tip to remember is to respect the patient’s privacy.
The patient cannot be forced to disclose information they are not comfortable with. Simply listening to whatever the patient says is another important tip to keep in mind. You may also see Work Assessment Form
What Is The Role of The Nurse?
The nurse is a comforting figure for a patient since the nurse is a person he or she interacts with the most during the stay in the hospital. A nurse fulfills important tasks in a patient’s care. You may also see Education Assessment Form
These tasks include the administration of assessment forms such as Community Assessment Form, evaluate the patient and family’s health status, develop an individual care plan for the patient for them to be to cope efficiently with their health condition, assures that the patient’s treatment goals are met, helps educate the patient on their health and condition, and conduct research which helps promote an evidence-based practice. You may also see Wellness Assessment Form
What is the Nursing Process?
In order to have the most effective and efficient patient care plan, a nurse must utilize advantageous methods to easily achieve this goal. One method a nurse typically goes for is the nursing process. The nursing process is considered to be a scientific method that aids in the assurance of having a high quality patient care. The nursing process consists of five phases. You may also see Income Assessment Form
The first phase is the assessment phase, which entails the collection of a patient’s information though the use of Health Assessment Forms. The second phase involves the diagnosis in relation to patient’s signs and symptoms. The third phase involves creating a plan for the patient’s care. The fourth phase is the implementation of the nurse’s plan of action. The last phase is the evaluation of the overall patient care from the nurse. You may also see Project Assessment Form
Why is nursing assessment important?
Nursing assessment is crucial for effective patient care. Key reasons include:
- Comprehensive Care: Ensures all aspects of patient health are considered.
- Early Detection: Identifies health issues early, like a Nutrition Assessment Form detects dietary deficiencies.
- Personalized Care: Tailors care plans to individual needs.
- Improved Outcomes: Enhances patient outcomes through accurate assessments.
- Professional Communication: Facilitates communication among the healthcare team. You may also see Financial Assessment Form
What is the Most Common Nursing Assessment?
The most common nursing assessment is the head-to-toe assessment, which systematically evaluates the patient’s entire body to identify health issues, similar to a comprehensive Health Assessment Form.
What is the Correct Order of Assessment in Nursing?
The correct order of assessment in nursing is inspection, palpation, percussion, and auscultation. This sequence ensures thorough examination, akin to following a structured Skills Assessment Form.
Can an RN Assess a Patient?
Yes, an RN (Registered Nurse) can assess a patient. They perform comprehensive evaluations, document findings, and develop care plans, much like completing a detailed Patient Assessment Form.
What is a Nursing Assessment Sheet?
A nursing assessment sheet is a tool used to record patient health information systematically. It includes sections for vital signs, symptoms, and medical history, similar to a Teacher Assessment Form.
What is a Nursing Assessment Checklist?
A nursing assessment checklist is a structured tool that guides nurses through essential steps for patient evaluation, ensuring all aspects are covered, much like a Preschool Assessment Form for early education.
How Do You Write a Nursing Assessment Note?
To write a nursing assessment note, document patient observations, symptoms, and vital signs clearly and concisely. Use a structured format similar to a Needs Assessment Form.
What is a Basic Nursing Assessment?
A basic nursing assessment includes evaluating vital signs, physical condition, and patient history to identify immediate health needs, akin to completing a Training Needs Assessment Form.
What is a Nursing Assessment in School?
A nursing assessment in school involves evaluating students’ health, identifying any medical issues, and creating care plans to support their well-being, similar to a Restaurant Risk Assessment Form for ensuring safety.
Related Posts
-
Enquiry Form
-
FREE 5+ Recruiter Performance Review Forms in PDF | MS Word
-
Job Safety Observation Form
-
FREE 4+ Hazard Observation Forms in PDF
-
FREE 5+ Coach Observation Forms in PDF | MS Word
-
FREE 4+ Child Care Observation Forms in MS Word | PDF
-
FREE 4+ Child Observation Forms in PDF | MS Word
-
Preschool Observation Form
-
Student Observation Form
-
Peer Observation Form
-
Lesson Observation Form
-
Content Retention Through Assessment Form [ How to, Importance, Tips ]
-
The Importance of Risk Assessment and Safety Statement [ What Is, How to Conduct ]
-
Risk Assessments And Safety Statements Guidelines [ What Is, Process ]
-
Choosing Careers Through Self Assessment [ What Is, Ways ]