
A Medical Record Form serves as the foundational document in healthcare, chronicling a patient’s medical history, treatments, and interactions with healthcare professionals. This crucial printable form, varying in type and design across healthcare settings, ensures consistency in patient care, provides vital information for diagnoses, and aids in medical research. Whether you’re a patient keen on understanding your health journey or a professional looking to optimize record-keeping, this guide delves into the meaning, types, examples, creation, and best practices of Medical Record Forms.
What is a Medical Record Form ? – Definition
A Medical Record Form is a systematic documentation of a patient’s medical history, treatments, diagnostic tests, consultations, and other interactions within a healthcare setting. This form, maintained by healthcare professionals, provides a comprehensive account of a patient’s health status, interventions, and outcomes over time. It serves as a communication tool among healthcare providers, ensuring continuity of care, and acts as a reference for medical decision-making, legal evidence, and health research.
What is the Meaning of a Medical Record Form?
The meaning of a Medical Record Form goes beyond its physical representation; it encapsulates a patient’s entire healthcare journey. It’s a chronological compilation of information detailing medical interventions, diagnoses, treatments, medications, allergies, radiology images, laboratory results, and notes from healthcare providers. This form offers healthcare professionals insights into a patient’s health history, ensuring informed and consistent care. Furthermore, it establishes a track record for potential future references, be it for clinical, legal, or research purposes, underpinning the continuity and quality of patient care.
What is the Best Sample Medical Record Form?
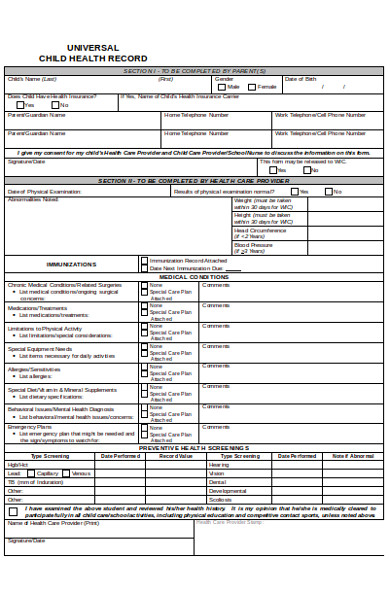
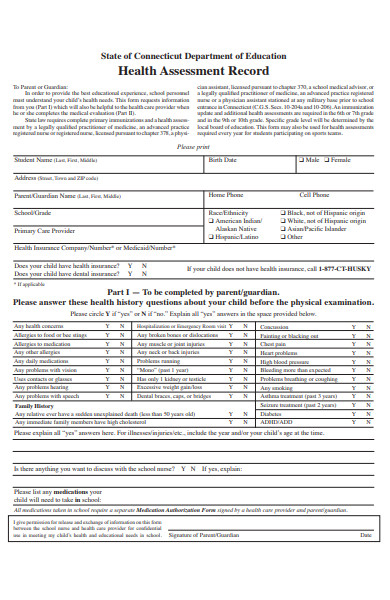
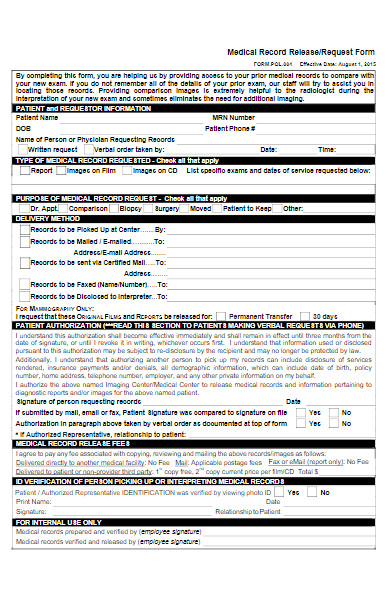
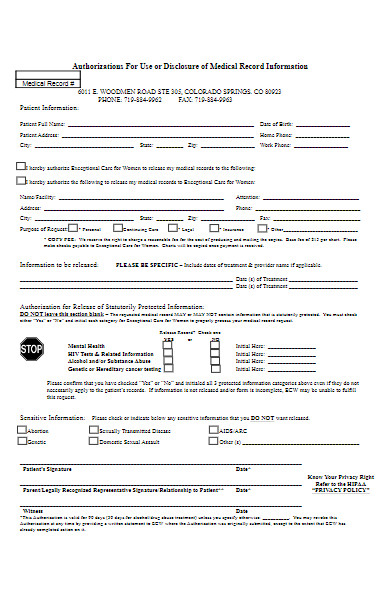
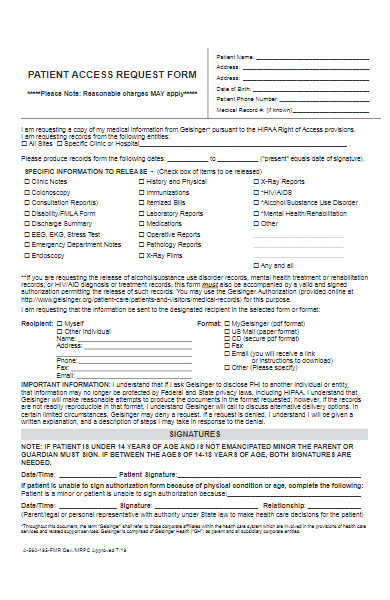
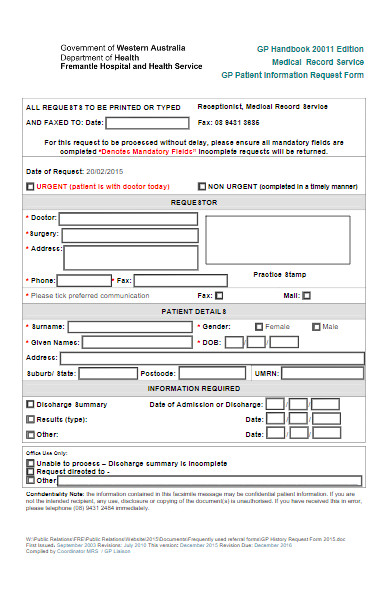
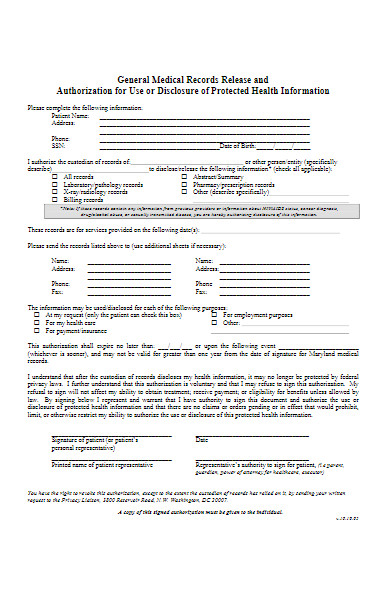
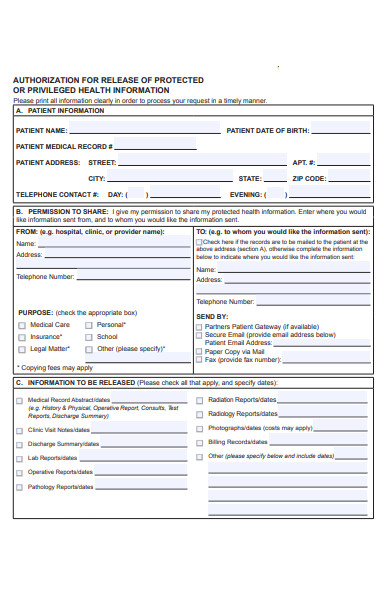
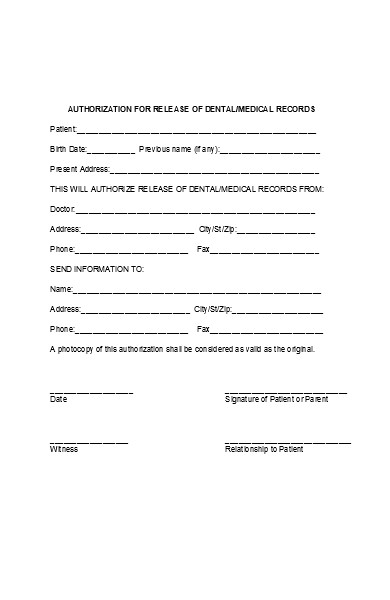
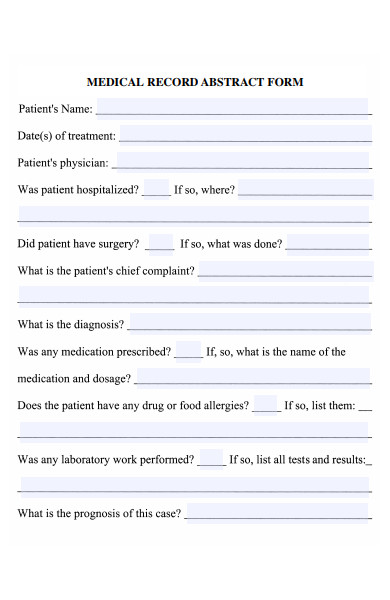
Providing a best sample Medical Record Form is challenging since the specifics often vary based on the healthcare setting, the country’s medical regulations, and the intended use of the form. However, a comprehensive Medical Record Form typically includes the following sections:
-
Patient Information:
- Full Name
- Date of Birth
- Gender
- Address
- Contact Number
- Emergency Contact
-
Medical History:
- Past illnesses or surgeries
- Current medications and dosages
- Allergies
- Immunization records
- Family medical history
-
Visit Details:
- Date of visit
- Reason for visit
- Diagnosis
- Treatment or medication prescribed
-
Lab and Test Results:
- Blood tests
- Radiology results, such as X-rays or MRIs
- Biopsy results, if applicable
-
Provider Notes:
- Observations during the visit
- Recommendations or future tests
- Referrals to specialists, if needed
-
Billing and Insurance Details:
- Insurance provider
- Policy number
- Billing details for the visit
-
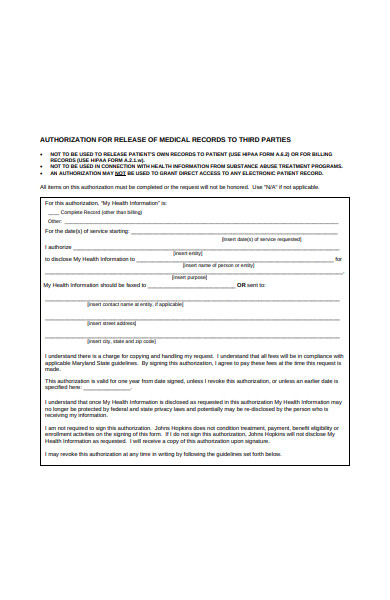
Consent Forms:
- For surgeries, treatments, or participation in research
-
Privacy Agreement:
- Acknowledging the patient’s rights and the institution’s commitment to maintaining confidentiality
-
Signature Section:
- Space for the medical professional’s signature to verify the details
It’s crucial to note that a patient’s medical record is confidential, and access is typically restricted to the patient and their authorized healthcare providers. Before using any sample information form, ensure it complies with local medical regulations, guidelines, and privacy laws.
FREE 35+ Medical Record Forms
What is a Medical Record Form used for?
A Medical Record Form is used to document a patient’s medical history, treatment plans, diagnoses, test results, medications, and other health-related information. This form serves multiple purposes:
- Continuity of Care: It provides healthcare professionals with a comprehensive view of the patient’s health, ensuring consistent and informed care.
- Communication: It allows for effective communication between different healthcare providers, especially if a patient sees multiple specialists.
- Legal Protection: It acts as evidence of patient care provided and can be essential in legal or malpractice cases.
- Billing and Insurance: It assists in processing insurance claims and ensuring accurate billing for services rendered.
- Research and Public Health: De-identified records can be used for medical research, understanding disease outbreaks, and public health interventions.
- Decision Making: It helps healthcare providers make informed decisions about patient care, treatment options, and potential interventions.
In essence, a Medical Record Form is a critical tool that ensures informed and safe patient care, facilitates communication among healthcare providers, and serves as an official patient’s report form with health and treatment history.
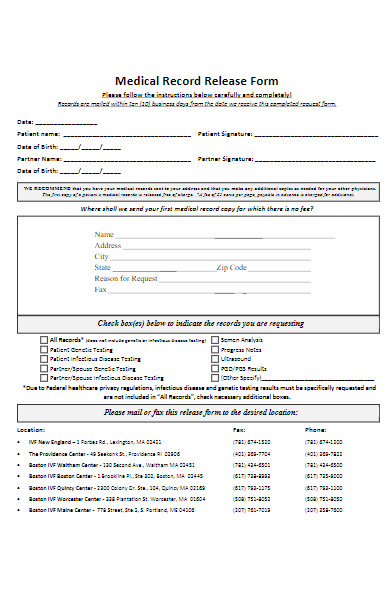
How do I request my Medical Record Form from a hospital?
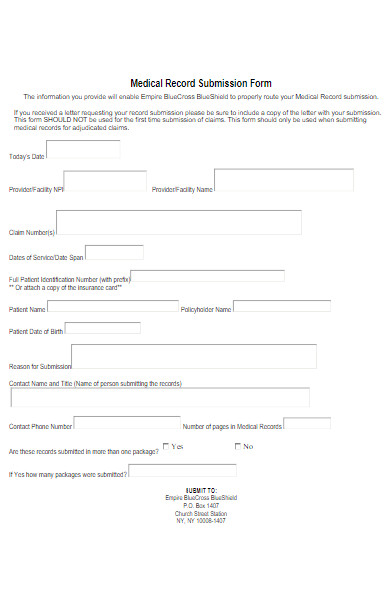
To request your Medical Record Form from a hospital, follow these general steps:
- Contact the Medical Records Department: Reach out to the hospital’s Medical Records or Health Information Management Department. They handle such requests.
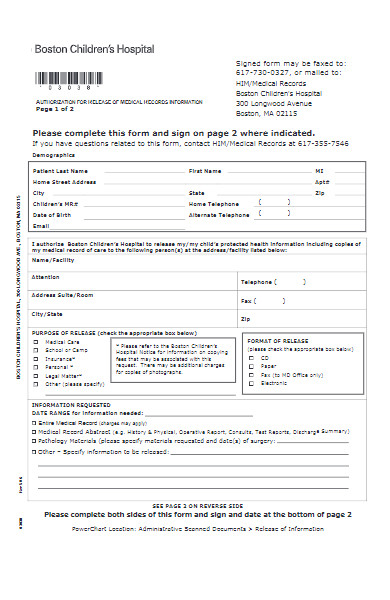
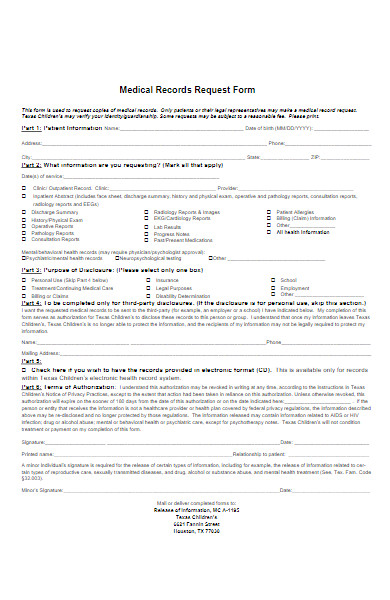
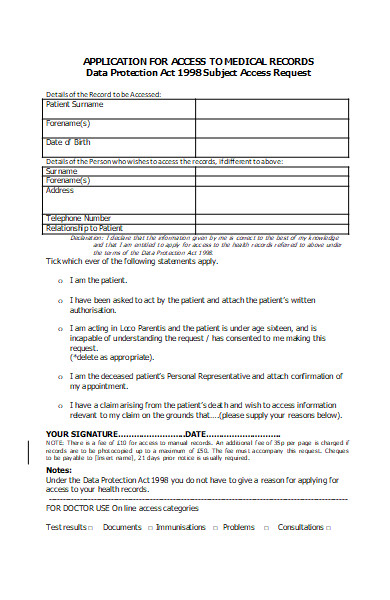
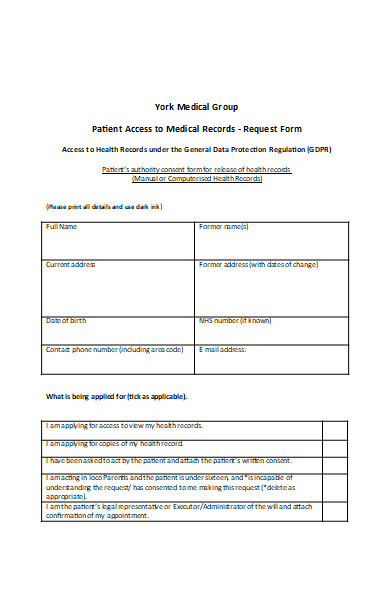
- Fill out a Request Form: Most hospitals require you to complete a specific authorization or release form to access your medical records. Ensure all details, like your full name, date of birth, and dates of treatment, are accurate.
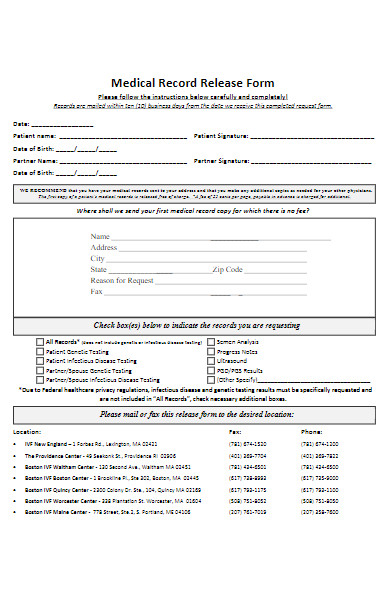
- Specify the Type of Records: Indicate whether you want the entire medical record or specific parts (e.g., lab reports, imaging studies, discharge summaries).
- Purpose of Request: Some forms might ask the reason for your request, such as transferring to a new physician, personal records, legal reasons, etc.
- Preferred Format: Indicate if you want a paper copy, digital copy (e.g., CD, USB, email), or if you’d like records sent directly to another healthcare provider.
- Submit the Form: This can usually be done in person, by mail, fax, or through a secure online portal, depending on the hospital’s protocol.
- Pay Associated Fees: While you have a right to your medical records, hospitals may charge a fee for copying and mailing. Some regions or states may regulate these fees.
- Wait: Once the request is submitted, it may take some time (often determined by local regulations) for the hospital to process it. For example, the U.S. Health Insurance Portability and Accountability Act (HIPAA) allows up to 30 days.
- Receive the Records: Once processed, you’ll receive your records in the format you specified.
- Review for Accuracy: Upon receiving your records, review them to ensure all information is accurate and complete.
Note: Procedures may vary slightly based on local regulations, the hospital’s policies, or the country in which you’re making the request. Always check the specific procedures of the hospital from which you’re requesting the records.
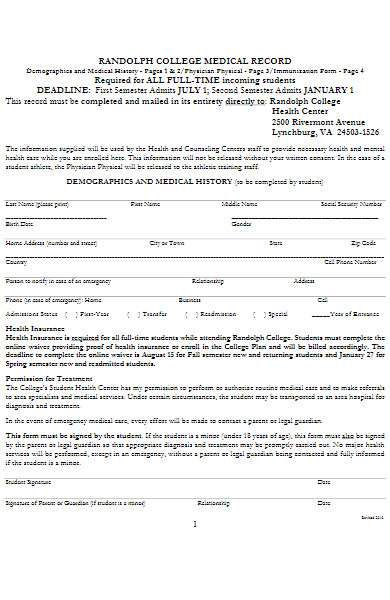
Can I access my child’s Medical Record Form without consent?
Generally, parents or legal guardians have the right to access their minor child’s medical records. However, there are exceptions and nuances to this rule, depending on the jurisdiction, the nature of the information, and other circumstances. Here’s a general overview:
- Parental Rights: Parents or legal guardians usually have the right to access their minor child’s medical records. This is because they are typically responsible for making healthcare decisions on the child’s behalf.
- Age of Consent: In some jurisdictions, once a child reaches a certain age (often termed the “age of medical consent”), they might have rights to keep parts or all of their medical records private from their parents.
- Sensitive Information: Depending on local laws, there may be restrictions on parental access to certain types of information, such as sexual health, mental health, substance use treatment, or reproductive health services.
- Child’s Consent: In some cases, if a minor can understand the implications of their rights to privacy, they may be allowed to give or withhold consent to share their medical information.
- Legal Situations: In cases where parental rights have been terminated or restricted due to legal reasons, access to a child’s medical records may be limited or denied.
- Privacy Laws: Regulations such as the U.S. Health Insurance Portability and Accountability Act (HIPAA) outline specific guidelines and exceptions regarding a parent’s access to a child’s medical records.
- Emancipated Minors: If a child is legally emancipated, they typically have the same rights as an adult, meaning parents may not have automatic access to their medical records.
It’s essential to consult with the healthcare provider or the medical facility’s records department to understand the specifics. Additionally, always be aware of local and national laws and regulations that might apply to your particular situation. You should also take a look at our Health Record form.
How long should I keep my Medical Record Form?
The length of time you should keep your Medical Record Form can vary based on several factors, including legal requirements, medical considerations, and personal preference. Here’s a general guideline:
- Legal Requirements: Depending on your jurisdiction, there might be laws that dictate how long medical records should be retained. For instance, in many places, healthcare providers are required to keep adult patients’ medical records for at least six to ten years from the date of the patient’s last visit. For minors, records might be retained until the child turns a specific age, often age 21.
- Chronic Conditions: If you have a chronic medical condition, it’s a good idea to keep all relevant medical records indefinitely. They can provide a comprehensive history that may be helpful in future treatment decisions.
- Major Surgeries or Significant Health Events: Records of surgeries, significant treatments, or diagnoses should be kept indefinitely, as they might be relevant to future medical care or decisions.
- Vaccination Records: Keep vaccination records indefinitely. They can be crucial for travel, school admissions, and some employment situations.
- Billing and Insurance: Retain any medical billing records until you’re sure that all claims have been settled and paid. Typically, this would be for at least one year.
- Medications: It’s helpful to keep a list of past and current medications, including any adverse reactions, as this can be relevant information for healthcare providers.
- Personal Preference: Some individuals prefer to keep all medical records as a comprehensive health history, especially in the age of digital storage where physical space isn’t a concern.
- Transitioning Providers: If you’re transitioning to a new healthcare provider, it’s helpful to have your records, at least from the past few years, to ensure continuity of care.
Remember, while you might have personal copies of your Medical Record Form, healthcare providers also keep their copies based on legal and professional guidelines. However, it’s always a good practice to have your records, especially for significant events or treatments, to ensure you have access to your health history whenever needed. Our Medical Records Transfer Forms is also worth a look at
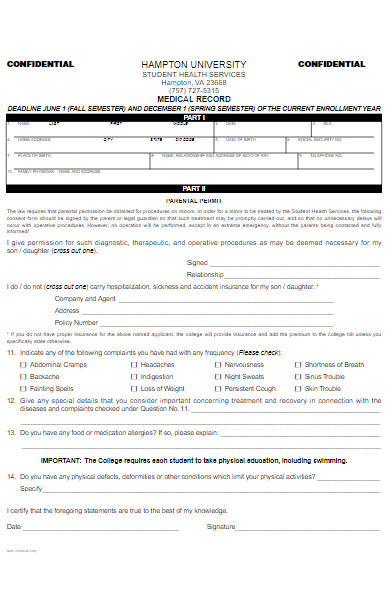
What details are typically included in a Medical Record Form?
A Medical Record Form serves as a comprehensive documentation of a patient’s health history and interactions with healthcare providers. Here are the typical details included in such a form:
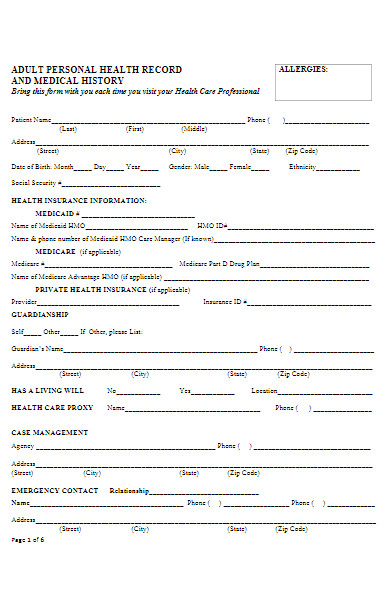
- Patient Demographics: This includes the patient’s full name, date of birth, address, contact numbers, emergency contact, and sometimes other identifiers like Social Security Number or patient ID.
- Medical History: Detailed information about past diseases, surgeries, hospitalizations, allergies, and any chronic conditions.
- Family Medical History: Information about diseases or conditions that have a genetic predisposition or are common in the patient’s family.
- Medications: A list of current and past medications, including dosage, frequency, and duration. This also includes any known drug allergies or adverse drug reactions.
- Consultation Notes: Notes from doctors, nurses, therapists, and other healthcare professionals from each visit or consultation.
- Diagnoses: All medical diagnoses the patient has received.
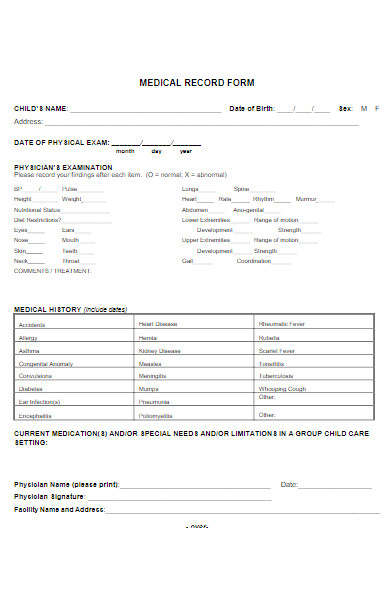
- Lab and Test Results: This includes blood tests, imaging studies (like X-rays, MRIs, CT scans), biopsies, and any other diagnostic test results.
- Treatment Plans: Information on prescribed treatments, surgeries, therapies, and interventions, including their dates and outcomes.
- Immunizations: A record of all vaccines received, including dates.
- Billing Information: Details related to the financial aspect of treatments, including insurance information, billing details, and payment history.
- Advance Directives: Documents that state a patient’s wishes for end-of-life care, like living wills or durable power of attorney for healthcare.
- Consent Forms: Signed documents where the patient (or guardian) has given permission for specific treatments, procedures, or participation in clinical trials.
- Discharge Summaries: Detailed notes provided when a patient is discharged from a hospital or facility, outlining the care received and recommendations for follow-up care.
- Correspondence: Any relevant communication between healthcare providers or with the patient.
- Growth and Development Records: Especially for pediatric patients, these track a child’s growth, developmental milestones, and any pertinent screenings.
- Behavioral and Mental Health Notes: Information related to mental and emotional well-being, therapies, and interventions.
The specific details captured can vary based on the medical facility, the nature of the visit, the healthcare system of a country, and the specialty of the healthcare provider. However, the primary objective remains consistent: to provide a thorough and continuous record of a patient’s health and medical care. In addition, you should review our Medical Records Request Form.
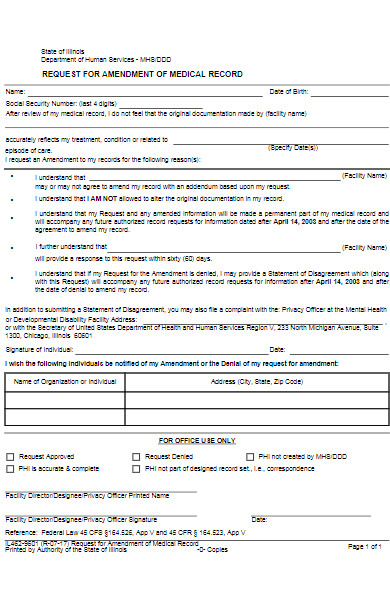
How do I correct an error on my Medical Record Form?
Correcting an error on your Medical Record Form is essential to ensure that you receive appropriate medical care based on accurate information. Here’s a step-by-step process to address errors:
- Review Your Records Regularly: Periodically request and review copies of your medical records to ensure that all information is accurate.
- Identify the Error: Clearly note the incorrect information. It can be helpful to provide a copy of the relevant page with the error highlighted or circled.
- Contact the Medical Records Department: Most healthcare facilities have a Medical Records or Health Information Management Department. Contact them and explain the error you’ve found. They can provide guidance on the facility’s specific process for making corrections.
- Submit a Formal Request: If the healthcare provider agrees that there’s an error, they might ask you to submit a formal written request detailing the incorrect information and providing the correct information. Ensure this request is dated, and keep a copy for your records.
- Provide Supporting Documentation: In some cases, especially if there’s a dispute about the accuracy of the information, you may need to provide supporting documentation. This could include records from other healthcare providers, lab results, or anything else that verifies the correct information.
- Follow Up: After submitting your request, follow up to check on the status. Corrections might not be immediate, so it’s essential to be proactive.
- Amendment vs. Correction: Instead of changing the original record, many healthcare providers will add an amendment or an addendum to the record that provides the correct information. This ensures that there’s a continuous record of all information (even if some of it was incorrect) and any changes made.
- Rights Under Law: In some regions or countries, you have legal rights concerning the correction of your medical records. For example, in the U.S., the Health Insurance Portability and Accountability Act (HIPAA) gives patients the right to request corrections to their medical records. However, healthcare providers can deny these requests under certain conditions.
- Disputes: If a healthcare provider denies your request to correct an error, they must provide a written explanation for the denial. You can then submit a written statement of disagreement that will be added to your medical record.
- Notify Other Healthcare Providers: If incorrect information was shared with other healthcare providers or entities (like insurance companies), request that the facility where the error originated notify them of the correction.
Errors in medical records can have significant implications, so it’s crucial to be proactive in ensuring your information is accurate. If you face challenges in correcting an error, consider seeking advice or assistance from patient advocacy groups or legal counsel. You may also be interested in our Sample Medical Records Release Form.
Can insurance companies access my Medical Record Form?
Yes, insurance companies can access certain parts of your Medical Record Form, but there are conditions and regulations governing this access:
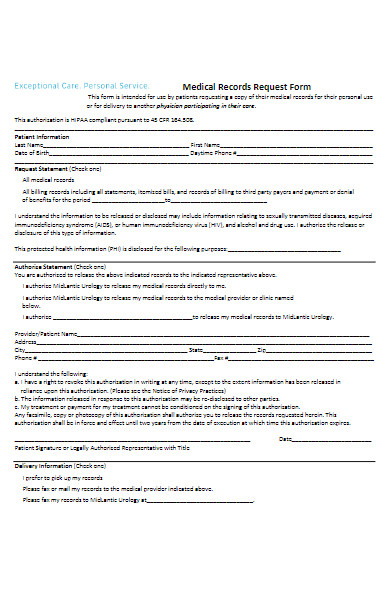
- Consent is Key: Insurance companies usually require your explicit consent to access your medical records. This consent is often part of the application process when you apply for health, life, or disability insurance. By signing the application or a specific authorization form, you’re granting the insurance company permission to request and review your medical records.
- Purpose of Access: Insurance companies might access your medical records for various reasons, including:
- Underwriting: When you apply for health, life, or disability insurance, insurers might review your medical history to determine the level of risk you pose. This can affect whether they offer you a policy and at what premium.
- Claims Processing: If you file a claim, especially for disability or a health issue, the insurance company may review your medical records to verify the claim’s legitimacy.
- Policy Renewal: In some cases, insurers might revisit your medical records when a policy is up for renewal, especially if conditions have changed.
- HIPAA Regulations (U.S. Specific): In the United States, the Health Insurance Portability and Accountability Act (HIPAA) sets strict standards for sharing health information. While you might grant an insurance company access to your records, your healthcare providers are still obligated under HIPAA to protect your information and only share it under the conditions you’ve approved.
- Limitations on Access: You can specify which parts of your medical records the insurance company can access. For example, you might allow them to view records related to a specific condition or time period but not your entire medical history. However, limiting access might affect the insurance company’s decision-making process.
- Rights to Deny or Revoke Access: In some jurisdictions, you might have the right to deny or revoke an insurance company’s access to your medical records. However, doing so could impact your insurance application or claim.
- Medical Information Bureau (MIB): In North America, the MIB operates as an information exchange between member insurance companies. If you’ve previously applied for life, health, or disability insurance and underwent underwriting, information about you might be stored in the MIB’s database. This doesn’t include detailed medical records but can have coded reports indicating medical conditions or risky behaviors. Insurance companies might check this database during the underwriting process.
- Potential Misuse: If you believe an insurance company accessed your medical records without proper authorization or misused your information, you might have legal recourse. It’s essential to know your rights and the regulations in your jurisdiction.
In summary, while insurance companies can access your Medical Record Form, there are rules and regulations in place to protect your privacy. Always read any authorization forms thoroughly before signing and understand your rights concerning your medical information. You can also refer to our Medical Forms.
How secure is my data on a digital Medical Record Form?
The security of data on a digital Medical Record Form (often referred to as Electronic Health Records or EHRs) is of paramount importance, given the personal and sensitive nature of health information. Various measures are in place to ensure the safety of this data:
- Regulations and Compliance: Many countries have established strict regulations to safeguard electronic medical records. In the U.S., for instance, the Health Insurance Portability and Accountability Act (HIPAA) sets standards for the protection of electronic health information, and institutions must adhere to these standards or face significant penalties.
- Encryption: Digital Medical Record Forms are typically encrypted, both when stored (at rest) and when being transmitted (in transit). Encryption transforms the data into a code to prevent unauthorized access.
- Access Controls: Only authorized personnel have access to EHRs. This is managed through authentication mechanisms such as passwords, PINs, biometrics, or smart cards. Role-based access further ensures that individuals can only access the data necessary for their job functions.
- Audit Trails: Modern EHR systems maintain detailed logs of all access and actions taken on a record. This means that any unauthorized access or changes can be traced back to a specific user and time.
- Data Backup: Regular backups ensure that medical data can be restored in case of events like system failures or data corruption. These backups are often encrypted and stored securely, sometimes in off-site locations.
- Firewalls and Intrusion Detection Systems: These act as barriers to prevent malicious activities and unauthorized access. They monitor and control incoming and outgoing network traffic based on predetermined security policies.
- Regular Updates and Patches: EHR software providers routinely release updates to address known vulnerabilities. It’s crucial for healthcare providers to apply these patches promptly to maintain the security of their systems.
- Physical Security: In addition to digital safeguards, data centers storing electronic medical records usually have physical security measures, including surveillance cameras, biometric access controls, and security personnel.
- Training: Healthcare employees are frequently trained on the importance of data security, emphasizing the need to follow best practices and report any suspicious activities.
- Data Integrity Measures: These ensure that the data remains accurate and unchanged unless modifications are made by authorized users.
Despite these security measures, no system is entirely immune from risks. Breaches can and do happen, often due to human errors, such as weak passwords or falling victim to phishing attacks. As a patient, it’s essential to be proactive: inquire about the security measures in place at your healthcare provider and ensure you’re following recommended practices when accessing your health information form online.
In conclusion, while robust measures are in place to secure digital Medical Record Forms, continuous efforts, technology advancements, and vigilance are essential to protect against evolving threats.
How to Create a Medical Record Form?
Creating a Medical Record Form requires a thoughtful approach to ensure all relevant details are captured, and the form is user-friendly for both patients and healthcare professionals. Here’s a step-by-step guide:
1. Define the Purpose:
Determine the specific purpose of the form. Are you creating it for new patient intake, updating existing records, or a specific medical examination?
2. Gather Basic Patient Information:
Include fields for:
- Full name
- Date of birth
- Gender
- Address
- Contact number(s)
- Email address
- Emergency contact details
3. Medical History:
- Current Medical Conditions: List of ongoing medical issues.
- Previous Medical Conditions: Past illnesses or surgeries.
- Medications: Current and past, including dosages.
- Allergies: Medications, foods, environmental factors, etc.
4. Family Medical History:
Document any known hereditary conditions or diseases that run in the family.
5. Lifestyle Information:
Details such as smoking, alcohol consumption, physical activity levels, diet, and any recreational drug use.
6. Current Complaints or Concerns:
Provide space for patients to write current symptoms or medical concerns.
7. Vaccination Record:
Details of immunizations received, including dates.
8. Insurance Details:
Information about the patient’s insurance provider, policy number, and other relevant data.
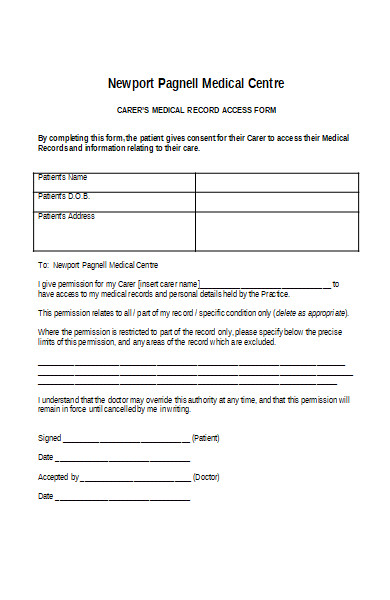
9. Consent and Authorization:
Include a section where the patient authorizes the release or request of medical records from/to other healthcare providers.
10. Privacy and Confidentiality Statement:
Ensure that patients understand their rights to privacy and how their information will be used.
11. Signature and Date:
Spaces for both the patient and the healthcare provider to sign and date the form, confirming the accuracy of the information.
12. Design and Layout:
- Use clear headings and subheadings.
- Avoid medical jargon; use layman’s terms when possible.
- Ensure enough spacing between lines for legible handwriting.
- Consider checkboxes for common conditions or yes/no questions to make filling out faster.
13. Test the Form:
Before finalizing, test the form with a few patients or colleagues to get feedback. This will help you identify any missing elements or sections that might be confusing.
14. Digital Integration (if applicable):
If you’re using an Electronic Health Record (EHR) system, ensure that the form can be integrated or uploaded into the system. Consider creating a digital version of the form for online submissions.
15. Review and Update:
Regularly review the form to ensure it remains up-to-date with medical best practices and regulatory requirements.
16. Maintain Security:
If the fillable form is digital, ensure it’s encrypted and compliant with data protection regulations. For physical forms, maintain them in a secure location.
In conclusion, the creation of a Medical Record Form requires thoroughness and attention to detail. Regularly updating the form based on feedback and changes in the medical field will ensure its continued effectiveness and relevance.
Tips for creating an Effective Medical Record Form
Creating an effective Medical Record Form involves ensuring it’s comprehensive, user-friendly, and safeguarded. Here are some tips to keep in mind:
- Simplicity is Key: Make sure the form is easy to understand. Use clear language and avoid jargon. This helps patients provide accurate information without confusion.
- Logical Flow: Organize sections in a logical order, such as starting with personal details, followed by medical history, then present complaints, etc.
- Use Standardized Terms: To avoid confusion, use standardized medical terms or classifications when listing conditions or treatments.
- Include Clear Instructions: Each section should have concise instructions or examples to guide the patient or medical staff.
- Leverage Technology: Consider using dropdown menus, checkboxes, and radio buttons in digital forms to speed up the process and minimize errors.
- Respect Privacy: Only request information that is essential. Make sure to include a privacy statement explaining how the patient’s information will be used and protected.
- Prioritize Legibility: If the form is to be filled out by hand, ensure there’s ample space for handwriting and consider using lined sections.
- Review Regularly: Medical practices and knowledge evolve. Regularly review and update the form to ensure it aligns with current practices.
- Include Visual Elements: When designing digital forms, use visual elements like icons or color-coded sections to guide users and make the form more engaging.
- Add a Review Section: A section at the end for patients or medical staff to review and confirm the accuracy of the information can be crucial.
- Consider Multi-Language Versions: Depending on the demographic of your patients, you might need the form to be available in multiple languages.
- Integrate with EHR Systems: If using a digital form, ensure it can integrate with Electronic Health Record systems to automate data input and reduce transcription errors.
- Use Durable Materials: If using paper forms, choose a quality paper that can withstand wear and tear, especially if the form will be handled frequently.
- Feedback Loop: Allow a mechanism for feedback on the form. This could be from medical staff or patients, ensuring continuous improvement.
- Security Measures: Ensure that both digital and physical forms have robust security measures in place. Digital forms should be encrypted, and physical forms should be stored securely.
- Backup Regularly: For digital forms, ensure there’s a regular backup process in place to prevent data loss.
- Training: Staff should be trained on how to guide patients in filling out the form and also on how to input or transfer this data into digital systems, if necessary.
By adhering to these tips, healthcare providers can create a Medical Record Form that not only captures all the necessary information but also offers an easy and efficient experience for both patients and staff.
A Medical Record Form is a crucial document, capturing comprehensive health data of an individual. It serves as an essential tool for healthcare providers, ensuring accurate diagnosis and treatment. Through understanding its meaning, types, and creation nuances, one can design an effective health form. With the proper approach and attention to detail, this form becomes an invaluable asset in patient care.
Related Posts
FREE 23+ Patient Release Forms in PDF MS Word
FREE 41+ Printable Medical Forms in PDF Excel | MS Word
FREE 8+ Sample BSA Medical Forms in PDF MS Word
FREE 11+ Medical Records Transfer Forms in PDF MS Word
FREE 9+ Sample Medical Records Release Forms in PDF MS ...
FREE 21+ Sample Medical Records Release Forms in PDF Word ...
FREE 37+ Blank Medical Forms in PDF MS Word | Excel
FREE 36+ Medical Forms in PDF MS Word | Excel
FREE 16+ Sample Medical Authorization Forms in PDF Word | Excel
10 Main Importance of Patient Registration Forms
FREE 7+ Sample Family Medical History Forms in MS Word PDF
FREE 6+ Medical History Forms in PDF MS Word | Excel
FREE 9+ Sample Medical Certification Forms in PDF MS Word
FREE 9+ Sample Medical Permission Forms in PDF MS Word
FREE 9+ Sample Medical Verification Forms in PDF MS Word